

Ionising radiation and cardiovascular disease: systematic review and meta-analysis
- PMID: 36889791
- PMCID: PMC10535030
- DOI: 10.1136/bmj-2022-072924
Ionising radiation and cardiovascular disease: systematic review and meta-analysis
Erratum in
-
Correction: Ionising radiation and cardiovascular disease: systematic review and meta-analysis.BMJ. 2025 Dec 12;391:r2557. doi: 10.1136/bmj.r2557. BMJ. 2025. PMID: 41386776 Free PMC article. No abstract available.
Abstract
Objective: To systematically review and perform a meta-analysis of radiation associated risks of cardiovascular disease in all groups exposed to radiation with individual radiation dose estimates.
Design: Systematic review and meta-analysis.
Main outcome measures: Excess relative risk per unit dose (Gy), estimated by restricted maximum likelihood methods.
Data sources: PubMed and Medline, Embase, Scopus, Web of Science Core collection databases.
Eligibility criteria for selecting studies: Databases were searched on 6 October 2022, with no limits on date of publication or language. Animal studies and studies without an abstract were excluded.
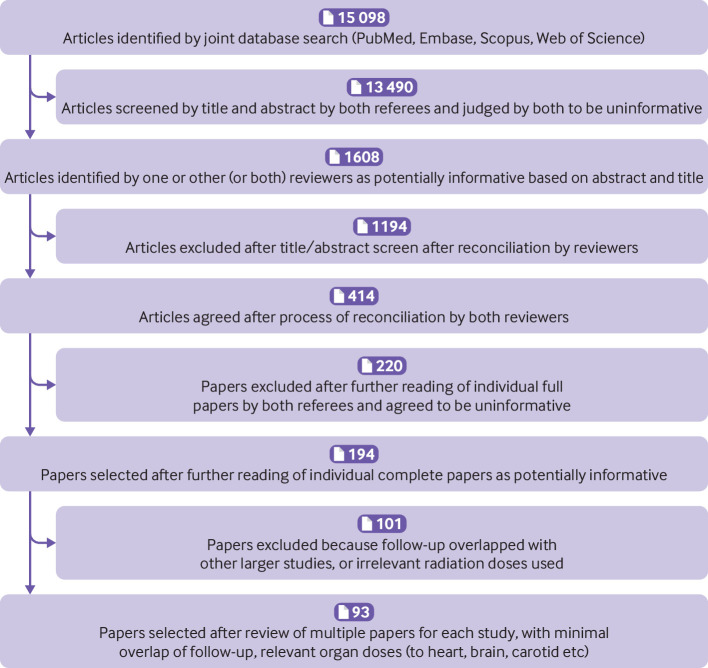
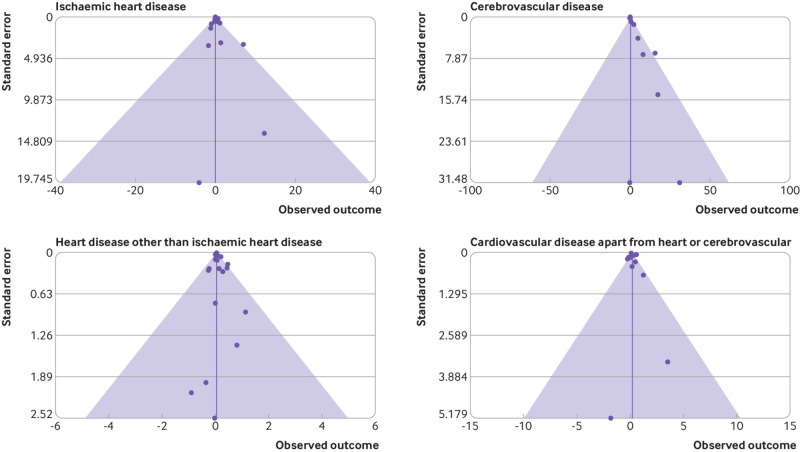
Results: The meta-analysis yielded 93 relevant studies. Relative risk per Gy increased for all cardiovascular disease (excess relative risk per Gy of 0.11 (95% confidence interval 0.08 to 0.14)) and for the four major subtypes of cardiovascular disease (ischaemic heart disease, other heart disease, cerebrovascular disease, all other cardiovascular disease). However, interstudy heterogeneity was noted (P<0.05 for all endpoints except for other heart disease), possibly resulting from interstudy variation in unmeasured confounders or effect modifiers, which is markedly reduced if attention is restricted to higher quality studies or those at moderate doses (<0.5 Gy) or low dose rates (<5 mGy/h). For ischaemic heart disease and all cardiovascular disease, risks were larger per unit dose for lower dose (inverse dose effect) and for fractionated exposures (inverse dose fractionation effect). Population based excess absolute risks are estimated for a number of national populations (Canada, England and Wales, France, Germany, Japan, USA) and range from 2.33% per Gy (95% confidence interval 1.69% to 2.98%) for England and Wales to 3.66% per Gy (2.65% to 4.68%) for Germany, largely reflecting the underlying rates of cardiovascular disease mortality in these populations. Estimated risk of mortality from cardiovascular disease are generally dominated by cerebrovascular disease (around 0.94-1.26% per Gy), with the next largest contribution from ischaemic heart disease (around 0.30-1.20% per Gy).
Conclusions: Results provide evidence supporting a causal association between radiation exposure and cardiovascular disease at high dose, and to a lesser extent at low dose, with some indications of differences in risk between acute and chronic exposures, which require further investigation. The observed heterogeneity complicates a causal interpretation of these findings, although this heterogeneity is much reduced if only higher quality studies or those at moderate doses or low dose rates are considered. Studies are needed to assess in more detail modifications of radiation effect by lifestyle and medical risk factors.
Systematic review registration: PROSPERO CRD42020202036.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interest: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: AJE has received speaker fees from Ionetix; has received consulting fees from WL Gore & Associates; has received authorship fees from Wolters Kluwer Healthcare–UpToDate; and has received grants to his institution from Attralus, Canon Medical Systems, Eidos Therapeutics, GE Healthcare, Pfizer, Roche Medical Systems, WL Gore & Associates, and XyloCor Therapeutics; none of these are related to the present work. Otherwise no other authors declare any competing interests.
Figures
Comment in
-
Increased cardiovascular disease risk after exposure to low dose radiation.BMJ. 2023 Mar 8;380:e074589. doi: 10.1136/bmj-2022-074589. BMJ. 2023. PMID: 36889793 No abstract available.
-
Authors' response to 'Estimates of cardiovascular disease risk from CT scans may be premature' (Harbron, 2024).J Radiol Prot. 2024 May 21;44(2). doi: 10.1088/1361-6498/ad4b28. J Radiol Prot. 2024. PMID: 38770739 No abstract available.
-
Estimates of cardiovascular disease risk from CT scans may be premature.J Radiol Prot. 2024 May 21;44(2). doi: 10.1088/1361-6498/ad4b27. J Radiol Prot. 2024. PMID: 38770744 No abstract available.
References
-
- World Health Organization (WHO). World Health Organization Statistical Information System (WHOSIS). Updated 17 November 2015. https://www.who.int/gho/en/. 2015.
-
- Centers for Disease Control and Prevention (CDC). CDC Wonder Atlanta, GA: Centers for Disease Control; 2020. https://wonder.cdc.gov/.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical