

Correction loss following short-segment posterior fixation for traumatic thoracolumbar burst fractures related to endplate and intervertebral disc destruction
- PMID: 36890495
- PMCID: PMC9993651
- DOI: 10.1186/s12891-023-06288-y
Correction loss following short-segment posterior fixation for traumatic thoracolumbar burst fractures related to endplate and intervertebral disc destruction
Abstract
Background: There has been widespread use of short-segment posterior fixation (SSPF) for traumatic thoracolumbar burst fractures. The relationship between the destruction of the vertebral endplate and adjacent disc and postoperative correction loss has been studied in only a few studies. This study investigated the risk factors for correction loss following SSPF.
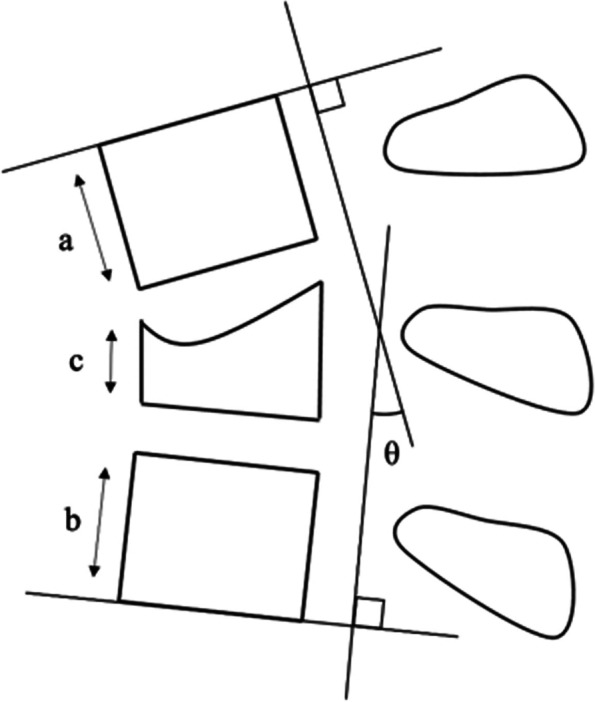
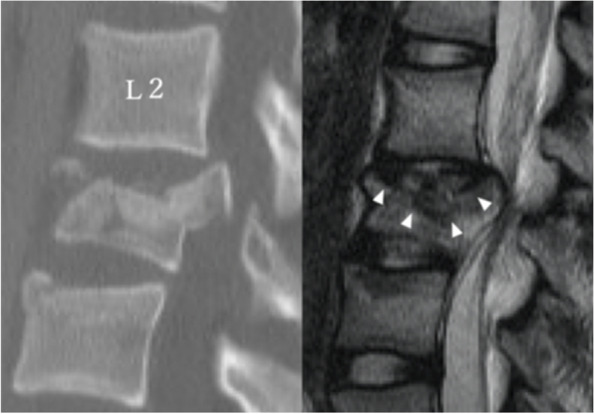
Methods: Forty-eight patients (mean age 35.0 years) who underwent SSPF for thoracolumbar burst fractures were enrolled. The mean follow-up period was 25.7 months (12-98 months). The neurological status and postoperative back pain were assessed by the medical records. Segmental kyphotic angle (SKA) and anterior vertebral body height ratio (AVBHR) were measured radiographically to assess indirect vertebral body reduction and local kyphosis. Preoperative Sander's traumatic intervertebral disc lesion (TIDL) classification and AO classification were used to evaluate the severity of disc and vertebral endplate injury. The corrective loss was considered present if ΔSKA was ≥10°. A multivariate logistic regression analysis was performed to identify the risk factors associated with postoperative loss of correction.
Results: The fracture distribution was as follows: 10 at T12, 17 at L1, 10 at L2, 9 at L3, and 2 at L4. Vertebral fractures were classified in the following way: A3 in 13 patients, A4 in 11, B1 in 11, and B2 in 13. In 47 patients (98%), a union of the fractured vertebrae was achieved. SKA and AVBHR improved significantly after surgery from 11.6° to 3.5° and from 67.2 to 90.0%, respectively. However, the correction loss at follow-up was 10.4° and 9.7%, respectively. Twenty patients (42%) had severe TIDL (grade 3). Postoperative ΔSKA and ΔAVBHR were significantly higher in patients with TIDL grade 3 than with TIDL grade 0-2. The presence of cranial TIDL grade 3 and older age were significant risk factors for ΔSKA ≥10° on multivariate logistic regression analysis. All patients could walk at follow-up. TIDL grade 3 and ΔSKA ≥10° were associated with severe postoperative back pain.
Conclusions: Risk factors for loss of correction after SSPF for thoracolumbar burst fractures were severe disc and endplate destruction at the time of injury and older age.
Keywords: Correction loss; Endplate injury; Short-segment posterior fusion; Thoracolumbar burst fractures; Traumatic intervertebral disk lesion.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Toyone T, Tanaka T, Kato D, Kaneyama R, Otsuka M. The treatment of acute thoracolumbar burst fractures with transpedicular intracorporeal hydroxyapatite grafting following indirect reduction and pedicle screw fixation: a prospective study. Spine (Phila Pa 1976) 2006;31:E208–E214. doi: 10.1097/01.brs.0000208161.74286.ad. - DOI - PubMed
-
- Knop C, Fabian HF, Bastian L, Blauth M. Late results of thoracolumbar fractures after posterior instrumentation and transpedicular bone grafting. Spine (Phila Pa 1976). 2001;(26):88–99. 10.1097/00007632-200101010-00016. - PubMed
-
- Aono H, Ishii K, Takenaka S, Tobimatsu H, Nagamoto Y, Horii C, Yamashita T, Furuya M, Iwasaki M. Risk factors for a kyphosis recurrence after short-segment temporary posterior fixation for thoracolumbar burst fractures. J Clin Neurosci. 2019;66:138–143. doi: 10.1016/j.jocn.2019.04.035. - DOI - PubMed
-
- Chen JX, Xu DL, Sheng SR, Goswami A, Xuan J, Jin HM, Chen J, Chen Y, Zheng ZM, Chen XB, Wang XY. Risk factors of kyphosis recurrence after implant removal in thoracolumbar burst fractures following posterior short-segment fixation. Int Orthop. 2016;40:1253–1260. doi: 10.1007/s00264-016-3180-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
