

Flavin fluorescence lifetime and autofluorescence optical redox ratio for improved visualization and classification of brain tumors
- PMID: 36890834
- PMCID: PMC9986542
- DOI: 10.3389/fonc.2023.1105648
Flavin fluorescence lifetime and autofluorescence optical redox ratio for improved visualization and classification of brain tumors
Abstract
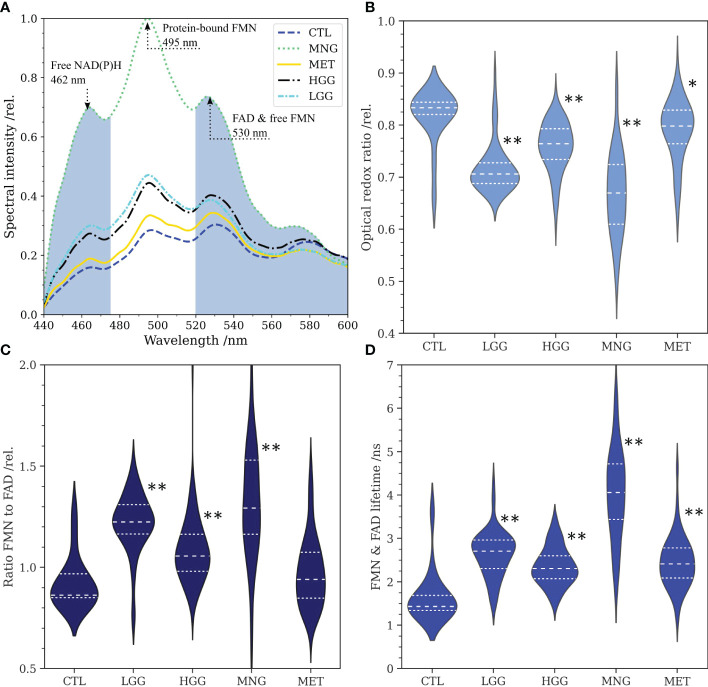
Purpose: Modern techniques for improved tumor visualization have the aim to maximize the extent of resection during brain tumor surgery and thus improve patient prognosis. Optical imaging of autofluorescence is a powerful and non-invasive tool to monitor metabolic changes and transformation in brain tumors. Cellular redox ratios can be retrieved from fluorescence emitted by the coenzymes reduced nicotinamide adenine dinucleotide (phosphate) (NAD(P)H) and flavin adenine dinucleotide (FAD). Recent studies point out that the influence of flavin mononucleotide (FMN) has been underestimated.
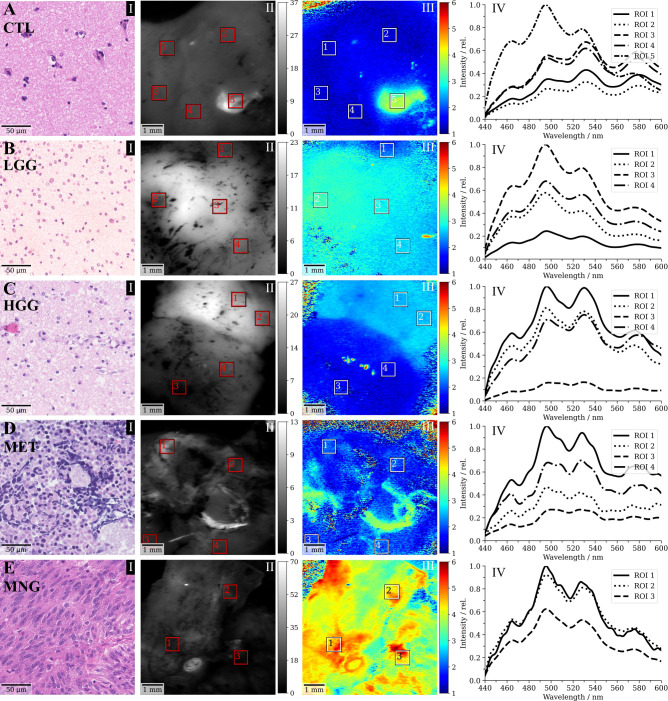
Experimental design: Fluorescence lifetime imaging and fluorescence spectroscopy were performed through a modified surgical microscope. We acquired 361 flavin fluorescence lifetime (500-580 nm) and fluorescence spectra (430-740 nm) data points on freshly excised different brain tumors: low-grade gliomas (N=17), high-grade gliomas (N=42), meningiomas (N=23), metastases (N=26) and specimens from the non-tumorous brain (N=3).
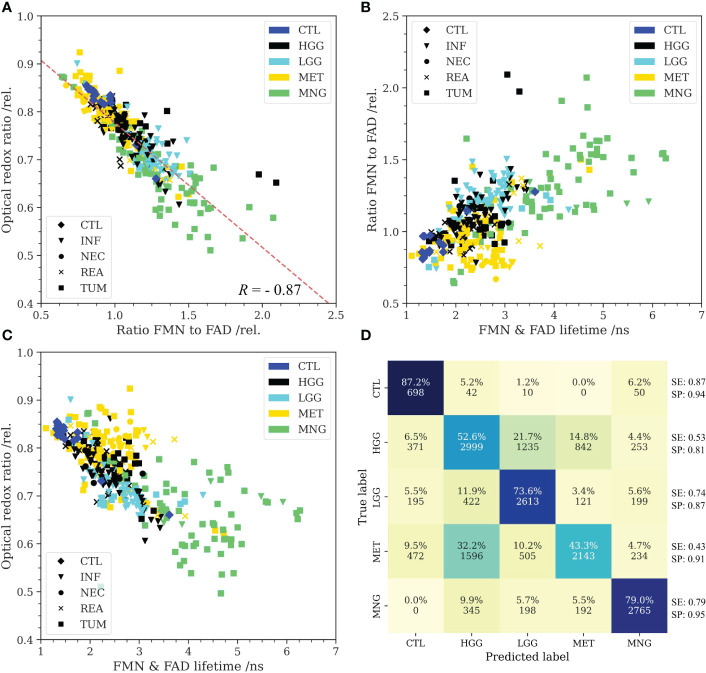
Results: Protein-bound FMN fluorescence in brain tumors did increase with a shift toward a more glycolytic metabolism (R=-0.87). This increased the average flavin fluorescence lifetime in tumor entities with respect to the non-tumorous brain. Further, these metrics were characteristic for the different tumor entities and showed promise for machine learning based brain tumor classification.
Conclusions: Our results shed light on FMN fluorescence in metabolic imaging and outline the potential for supporting the neurosurgeon in visualizing and classifying brain tumor tissue during surgery.
Keywords: flavin mononucleotide; fluorescence guided surgery; fluorescence lifetime imaging; fluorescence spectroscopy; optical redox ratio.
Copyright © 2023 Reichert, Wadiura, Erkkilae, Gesperger, Lang, Roetzer-Pejrimovsky, Makolli, Woehrer, Wilzbach, Hauger, Kiesel, Andreana, Unterhuber, Drexler, Widhalm and Leitgeb.
Conflict of interest statement
MW and CH are employees of Carl Zeiss Meditec AG, Oberkochen, Germany. GW received restricted travel grants from NX Development Corp. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Coburger J, Wirtz CR, König RW. Impact of extent of resection and recurrent surgery on clinical outcome and overall survival in a consecutive series of 170 patients for glioblastoma in intraoperative high field magnetic resonance imaging. J Neurosurg Sci (2017) 61(3):233–44. doi: 10.23736/S0390-5616.16.03284-7 - DOI - PubMed
LinkOut - more resources
Full Text Sources