

The impact of steerable sheath visualization during catheter ablation for atrial fibrillation
- PMID: 36891772
- PMCID: PMC10105886
- DOI: 10.1093/europace/euad029
The impact of steerable sheath visualization during catheter ablation for atrial fibrillation
Abstract
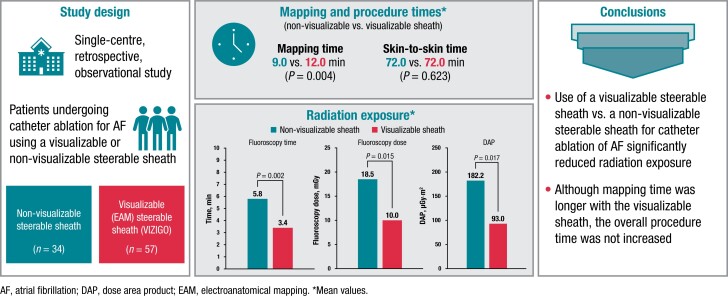
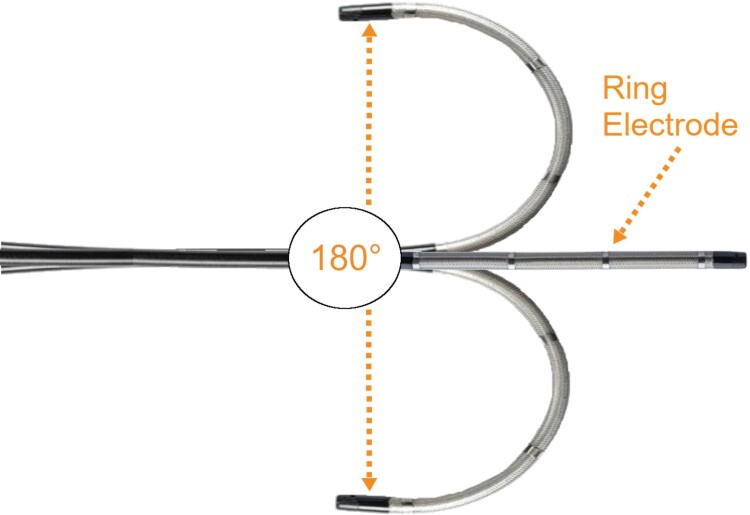
Aims: Incorporating a steerable sheath that can be visualized using an electroanatomical mapping (EAM) system may allow for more efficient mapping and catheter placement, while reducing radiation exposure, during ablation procedures for atrial fibrillation (AF). This study evaluated fluoroscopy usage and procedure times when a visualizable steerable sheath was used compared with a non-visualizable steerable sheath for catheter ablation for AF.
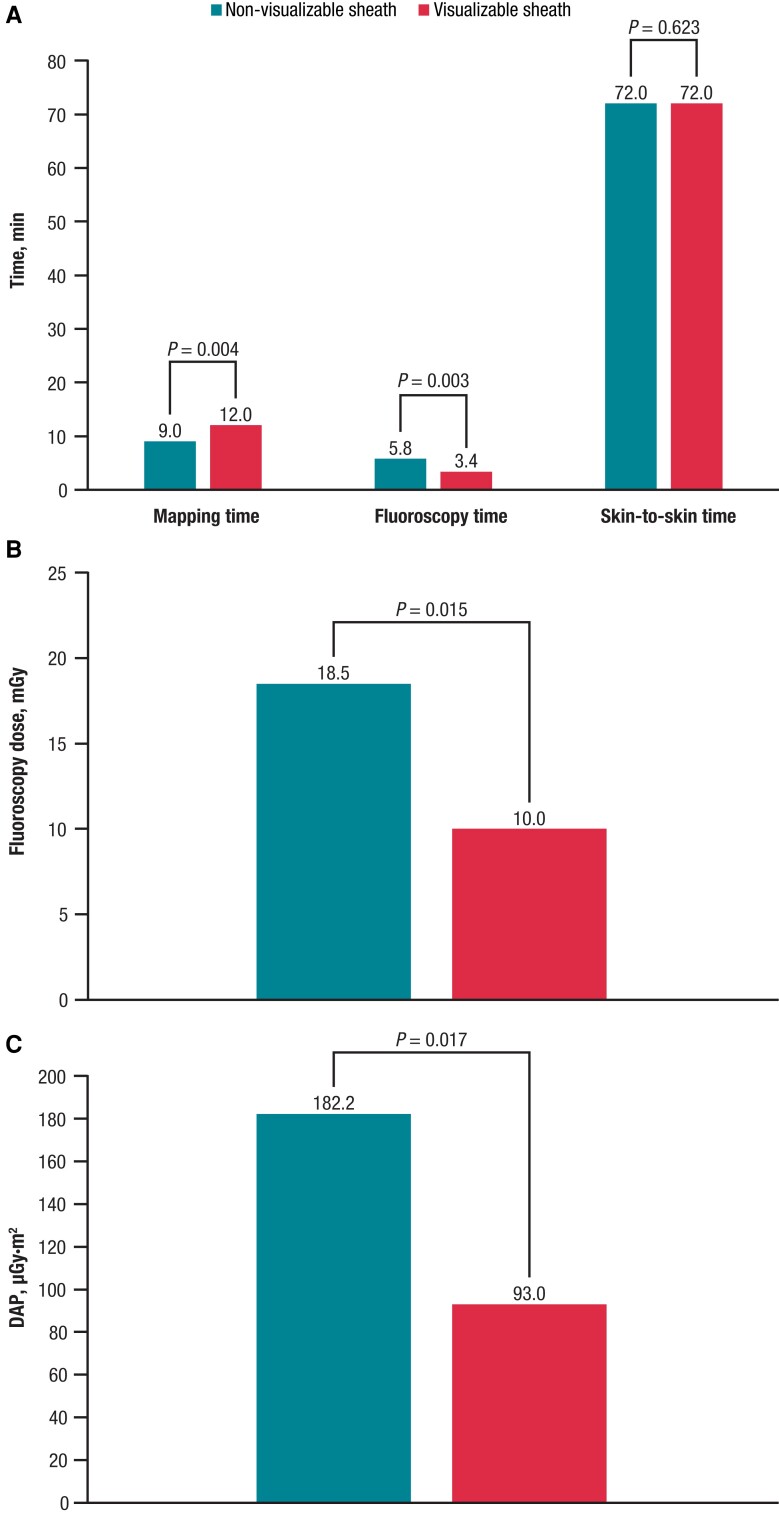
Methods and results: In this retrospective, observational, single-centre study, patients underwent catheter ablation for AF using a steerable sheath that is visualizable using the CARTO EAM (VIZIGO; n = 57) or a non-visualizable steerable sheath (n = 34). The acute procedural success rate was 100%, with no acute complications in either group. Use of the visualizable sheath vs. the non-visualizable sheath was associated with a significantly shorter fluoroscopy time [median (first quartile, third quartile), 3.4 (2.1, 5.4) vs. 5.8 (3.8, 8.6) min; P = 0.003], significantly lower fluoroscopy dose [10.0 (5.0, 20.0) vs. 18.5 (12.3, 34.0) mGy; P = 0.015], and significantly lower dose area product [93.0 (48.0, 197.9) vs. 182.2 (124.5, 355.0) μGy·m2; P = 0.017] but with a significantly longer mapping time [12.0 (9.0, 15.0) vs. 9.0 (7.0, 11.0) min; P = 0.004]. There was no significant difference between the visualizable and non-visualizable sheaths in skin-to-skin time [72.0 (60.0, 82.0) vs. 72.0 (55.5, 80.8) min; P = 0.623].
Conclusion: In this retrospective study, use of a visualizable steerable sheath for catheter ablation of AF significantly reduced radiation exposure vs. a non-visualizable steerable sheath. Although mapping time was longer with the visualizable sheath, the overall procedure time was not increased.
Keywords: Atrial fibrillation; Catheter ablation; Fluoroscopy time; Radiation protection; Visualizable sheath.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: N.F. reports institutional educational support from Biosense Webster and Synapse Medical as well as speakers fees from Daiichi Sankyo, unrelated to the submitted work. G.S. reports personal fees from Abbott, Bayer, Boston Scientific, and Biosense Webster Inc. outside the submitted work. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist Cet al. . 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373–498. - PubMed
-
- Van Der Zee SA, d’Avila A. Redo procedures in patients with paroxysmal atrial fibrillation. J Innov Card Rhythm Manag 2010;1:44–52.
-
- Muthalaly RG, John RM, Schaeffer B, Tanigawa S, Nakamura T, Kapur Set al. . Temporal trends in safety and complication rates of catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol 2018;29:854–60. - PubMed
-
- Deneke T, Schade A, Diegeler A, Nentwich K. Esophago-pericardial fistula complicating atrial fibrillation ablation using a novel irrigated radiofrequency multipolar ablation catheter. J Cardiovasc Electrophysiol 2014;25:442–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
