

Myocardial Revascularization in Patients With Ischemic Cardiomyopathy: For Whom and How
- PMID: 36892041
- PMCID: PMC10111551
- DOI: 10.1161/JAHA.122.026943
Myocardial Revascularization in Patients With Ischemic Cardiomyopathy: For Whom and How
Abstract
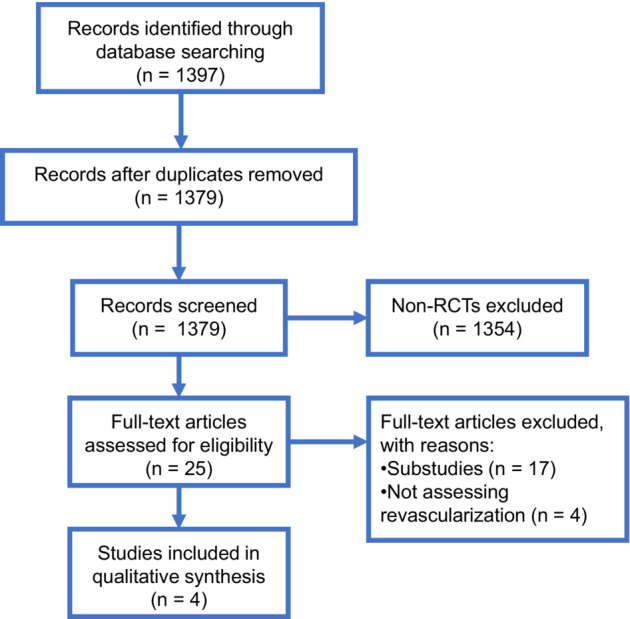
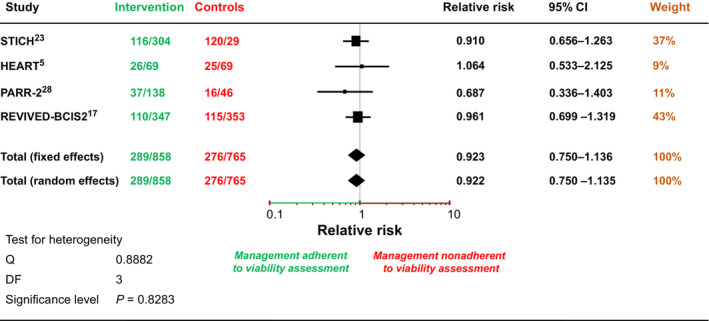
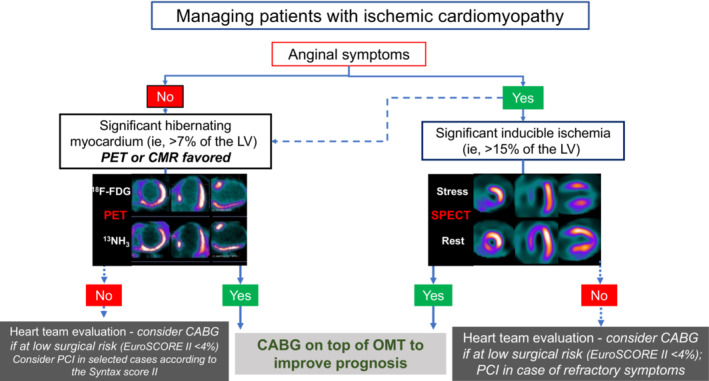
Background Myocardial revascularization has been advocated to improve myocardial function and prognosis in ischemic cardiomyopathy (ICM). We discuss the evidence for revascularization in patients with ICM and the role of ischemia and viability detection in guiding treatment. Methods and Results We searched for randomized controlled trials evaluating the prognostic impact of revascularization in ICM and the value of viability imaging for patient management. Out of 1397 publications, 4 randomized controlled trials were included, enrolling 2480 patients. Three trials (HEART [Heart Failure Revascularisation Trial], STICH [Surgical Treatment for Ischemic Heart Failure], and REVIVED [REVascularization for Ischemic VEntricular Dysfunction]-BCIS2) randomized patients to revascularization or optimal medical therapy. HEART was stopped prematurely without showing any significant difference between treatment strategies. STICH showed a 16% lower mortality with bypass surgery compared with optimal medical therapy at a median follow-up of 9.8 years. However, neither the presence/extent of left ventricle viability nor ischemia interacted with treatment outcomes. REVIVED-BCIS2 showed no difference in the primary end point between percutaneous revascularization or optimal medical therapy. PARR-2 (Positron Emission Tomography and Recovery Following Revascularization) randomized patients to imaging-guided revascularization versus standard care, with neutral results overall. Information regarding the consistency of patient management with viability testing results was available in ≈65% of patients (n=1623). No difference in survival was revealed according to adherence or no adherence to viability imaging. Conclusions In ICM, the largest randomized controlled trial, STICH, suggests that surgical revascularization improves patients' prognosis at long-term follow-up, whereas evidence supports no benefit of percutaneous coronary intervention. Data from randomized controlled trials do not support myocardial ischemia or viability testing for treatment guidance. We propose an algorithm for the workup of patients with ICM considering clinical presentation, imaging results, and surgical risk.
Keywords: coronary artery bypass surgery; hibernation; ischemic cardiomyopathy; myocardial ischemia; myocardial revascularization; myocardial viability; percutaneous coronary intervention.
Figures
References
-
- Cabac‐Pogorevici I, Muk B, Rustamova Y, Kalogeropoulos A, Tzeis S, Vardas P. Ischaemic cardiomyopathy. Pathophysiological insights, diagnostic management and the roles of revascularisation and device treatment. Gaps and dilemmas in the era of advanced technology. Eur J Heart Fail. 2020;22:789–799. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
