

Serum Pro-N-Cadherin Is a Marker of Subclinical Heart Failure in the General Population
- PMID: 36892069
- PMCID: PMC10111553
- DOI: 10.1161/JAHA.122.028234
Serum Pro-N-Cadherin Is a Marker of Subclinical Heart Failure in the General Population
Abstract
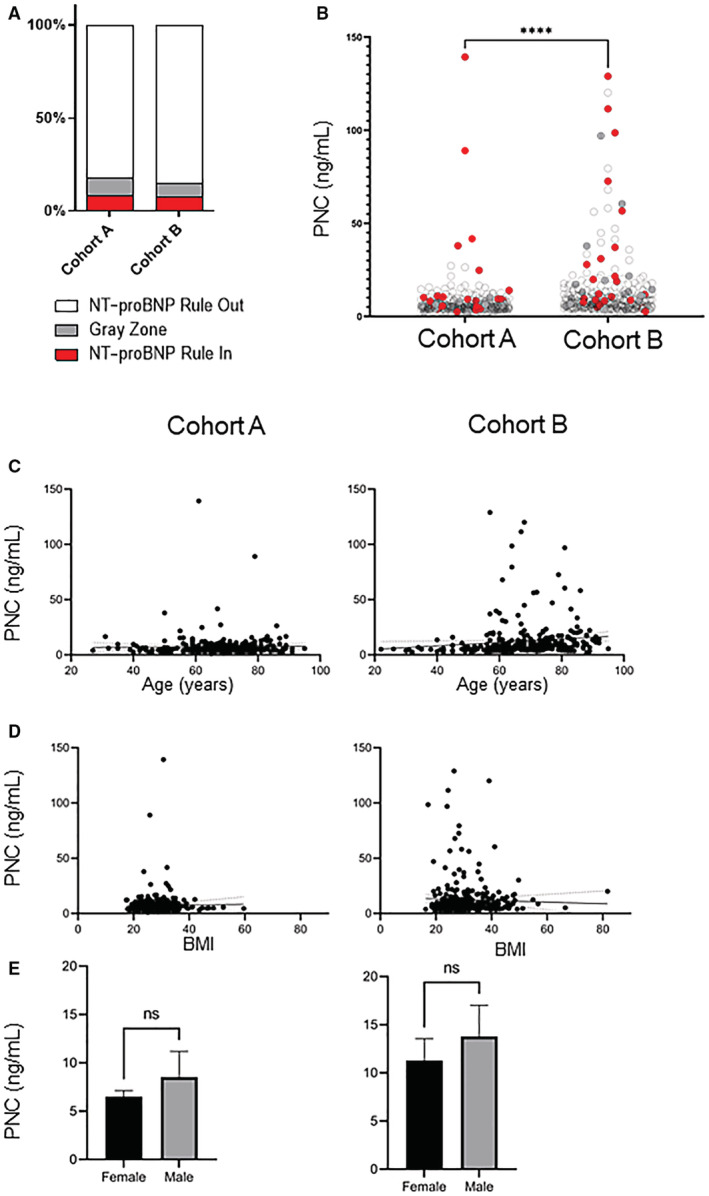
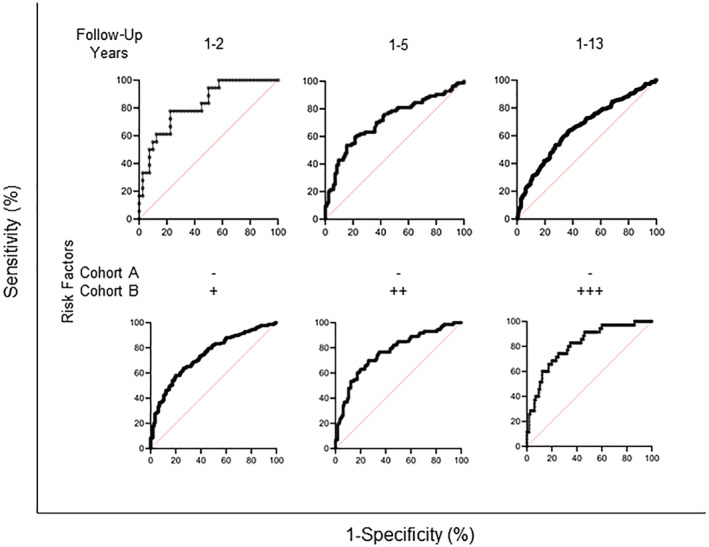
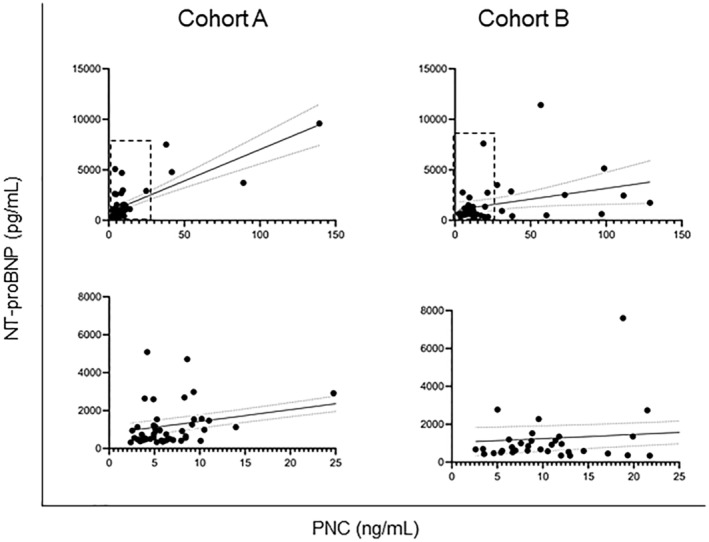
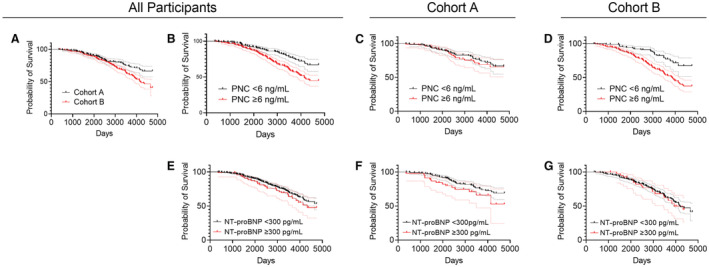
Background We recently reported aberrant processing and localization of the precursor PNC (pro-N-cadherin) protein in failing heart tissues and detected elevated PNC products in the plasma of patients with heart failure. We hypothesize that PNC mislocalization and subsequent circulation is an early event in the pathogenesis of heart failure, and therefore circulating PNC is an early biomarker of heart failure. Methods and Results In collaboration with the Duke University Clinical and Translational Science Institute's MURDOCK (Measurement to Understand Reclassification of Disease of Cabarrus and Kannapolis) study, we queried enrolled individuals and sampled 2 matched cohorts: a cohort of individuals with no known heart failure at the time of serum collection and no heart failure development in the following 13 years (n=289, cohort A) and a matching cohort of enrolled individuals who had no known heart failure at the time of serum collection but subsequently developed heart failure within the following 13 years (n=307, cohort B). Serum PNC and NT-proBNP (N-terminal pro B-type natriuretic peptide) concentrations in each population were quantified by ELISA. We detected no significant difference in NT-proBNP rule-in or rule-out statistics between the 2 cohorts at baseline. In participants who developed heart failure, serum PNC is significantly elevated relative to those who did not report development of heart failure (P<0.0001). Receiver operating characteristic analyses of PNC demonstrate diagnostic value for subclinical heart failure. Additionally, PNC has diagnostic potential when comparing participants with no reported heart failure risk factors from cohort A to at-risk participants from cohort B over the 13-year follow-up. Participants whose PNC levels measure >6 ng/mL have a 41% increased risk of all-cause mortality independent of age, body mass index, sex, NT-proBNP, blood pressure, previous heart attack, and coronary artery disease (P=0.044, n=596). Conclusions These data suggest that PNC is an early marker of heart failure and has the potential to identify patients who would benefit from early therapeutic intervention.
Keywords: BNP; NT‐proBNP; biomarkers; cardiovascular disease; heart failure; pro‐N‐cadherin.
Figures
References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2022;145:e895–e1032. doi: 10.1161/CIR.0000000000001063 - DOI - PubMed
-
- Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, Anker SD, Atherton J, Bohm M, Butler J, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and writing committee of the universal definition of heart failure: endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail. 2021;23:352–380. doi: 10.1002/ejhf.2115 - DOI - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez‐Sanchez MA, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–1847. doi: 10.1093/eurheartj/ehs104 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
