

Elevated levels of several chemokines in the cerebrospinal fluid of patients with subarachnoid hemorrhage are associated with worse clinical outcome
- PMID: 36893189
- PMCID: PMC9997919
- DOI: 10.1371/journal.pone.0282424
Elevated levels of several chemokines in the cerebrospinal fluid of patients with subarachnoid hemorrhage are associated with worse clinical outcome
Abstract
Background: Chemokines are small cytokines that exert chemotactic actions on immune cells and are involved in many inflammatory processes. The present study aims to provide insight in the role of this relatively unexplored family of proteins in the inflammatory pathophysiology of subarachnoid hemorrhage (SAH).
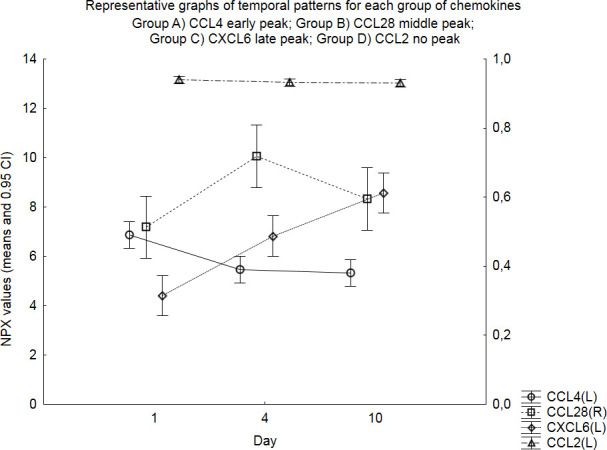
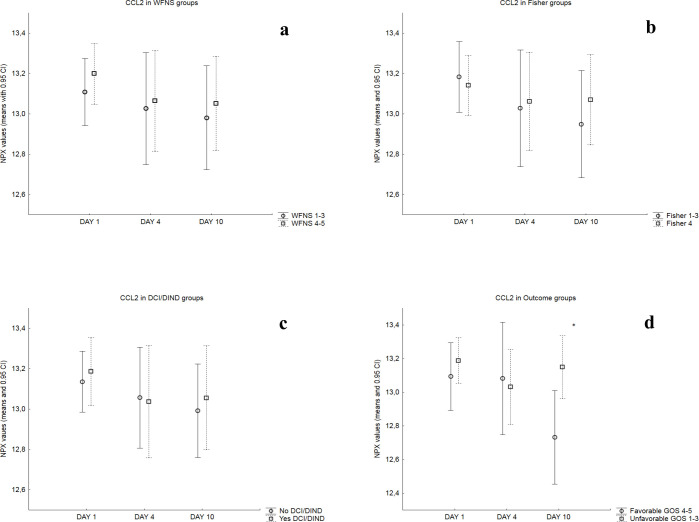
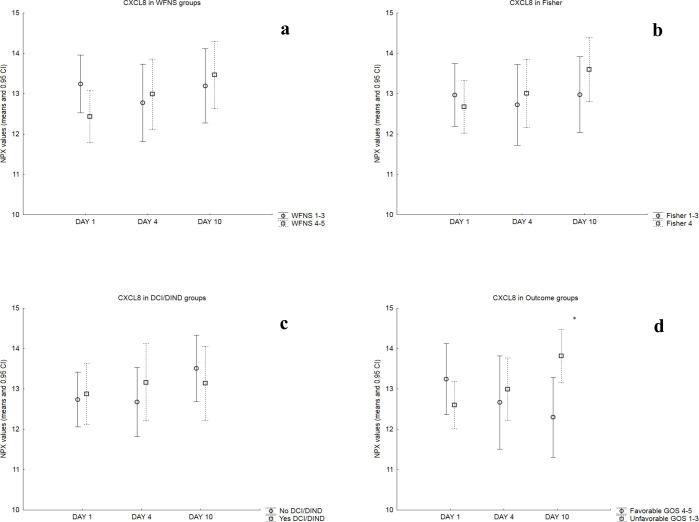
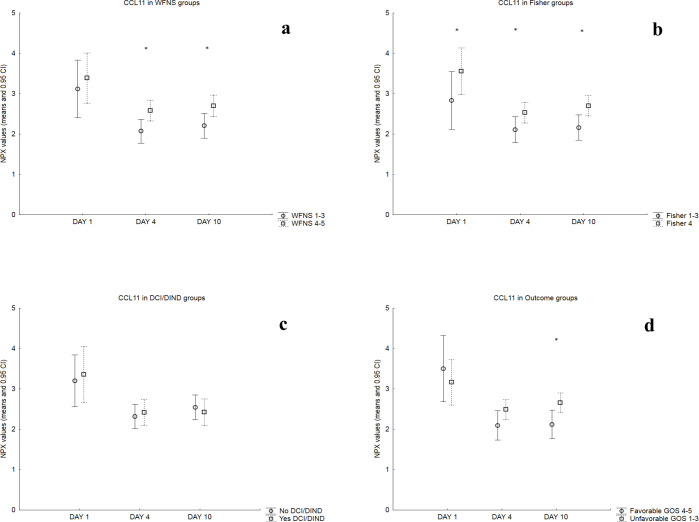
Materials and methods: Cerebrospinal fluid of 29 patients (17 female; mean age 57 years) was collected at days 1, 4 and 10 after SAH, centrifuged and frozen at -70°C. Analysis of 92 inflammation-related proteins was performed using Target 96 Inflammation ® assay (Olink Proteomics, Uppsala, Sweden) based on Proximity Extension Assay technology. The panel included 20 chemokines (CCL2 (or MCP-1), CCL3, CCL4, CCL7 (or MCP-3), CCL8 (or MCP-2), CCL11 (or Eotaxin), CCL13 (or MCP-4), CCL19, CCL20, CCL23, CCL25, CCL28, CXCL1, CXCL5, CXCL6, CXCL8 (or IL-8), CXCL9, CXCL10, CXCL11 and CX3CL1 (or Fractalkine)) that were analyzed for their temporal patterns of expression and compared in dichotomized clinical groups based on World Federation of Neurosurgical Societies (WFNS) admission score and amount of blood on admission CT based on Fisher scale; presence of delayed cerebral ischemia(DCI)/delayed ischemic neurological deficit (DIND); and clinical outcome based on Glasgow Outcome Scale. Protein expression levels were provided in output unit Normalized Protein Expression (NPX). ANOVA models were used for statistical analyses.
Results: Four temporal patterns of expression were observed (i.e., early, middle, late peak and no peak). Significantly higher day 10 mean NPX values were observed in patients with poor outcome (GOS 1-3) for chemokines CCL2, CCL4, CCL7, CCL11, CCL13, CCL19, CCL20, CXCL1, CXCL5, CXCL6 and CXCL8. In the WFNS 4-5 group, CCL11 showed significantly higher day 4 and day 10 mean NPX values and CCL25 significantly higher day 4 values. In patients with SAH Fisher 4, CCL11 showed significantly higher mean NPX values on days 1, 4 and 10. Finally, patients with DCI/DIND had significantly higher day 4 mean NPX values of CXCL5.
Conclusion: Higher levels of multiple chemokines at the late stage of SAH seemed to correlate with worse clinical outcome. A few chemokines correlated with WFNS score, Fisher score and occurrence of DCI/DIND. Chemokines may be useful as biomarkers for describing the pathophysiology and prognosis of SAH. Further studies are needed to better understand their exact mechanism of action in the inflammatory cascade.
Copyright: © 2023 Vlachogiannis et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Differential chemokine alteration in the variants of primary progressive aphasia-a role for neuroinflammation.J Neuroinflammation. 2021 Oct 3;18(1):224. doi: 10.1186/s12974-021-02247-3. J Neuroinflammation. 2021. PMID: 34602080 Free PMC article.
-
Chemokine profile in women with moderate to severe anxiety and depression during pregnancy.BMC Pregnancy Childbirth. 2021 Dec 4;21(1):807. doi: 10.1186/s12884-021-04225-2. BMC Pregnancy Childbirth. 2021. PMID: 34863117 Free PMC article.
-
Prognostic value of intrathecal heme oxygenase-1 concentration in patients with Fisher Grade III aneurysmal subarachnoid hemorrhage.J Neurosurg. 2014 Dec;121(6):1388-93. doi: 10.3171/2014.7.JNS131704. Epub 2014 Oct 3. J Neurosurg. 2014. PMID: 25280089
-
Effect of statin treatment on vasospasm-related morbidity and functional outcome in patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2017 Aug;127(2):291-301. doi: 10.3171/2016.5.JNS152900. Epub 2016 Oct 7. J Neurosurg. 2017. PMID: 27715439
-
Preclinical and clinical role of interleukin-6 in the development of delayed cerebral vasospasm and neuronal cell death after subarachnoid hemorrhage: towards a potential target therapy?Neurosurg Rev. 2022 Feb;45(1):395-403. doi: 10.1007/s10143-021-01628-9. Epub 2021 Aug 27. Neurosurg Rev. 2022. PMID: 34448990 Free PMC article. Review.
Cited by
-
IL-8 (CXCL8) Correlations with Psychoneuroimmunological Processes and Neuropsychiatric Conditions.J Pers Med. 2024 May 3;14(5):488. doi: 10.3390/jpm14050488. J Pers Med. 2024. PMID: 38793070 Free PMC article. Review.
-
Dual impact of neuroinflammation on cognitive and motor impairments in Alzheimer's disease.J Alzheimers Dis Rep. 2025 Jun 2;9:25424823251341870. doi: 10.1177/25424823251341870. eCollection 2025 Jan-Dec. J Alzheimers Dis Rep. 2025. PMID: 40463291 Free PMC article. Review.
-
Chronic immunosuppression across 12 months and high ability of acute and subacute CNS-injury biomarker concentrations to identify individuals with complicated mTBI on acute CT and MRI.J Neuroinflammation. 2024 Apr 27;21(1):109. doi: 10.1186/s12974-024-03094-8. J Neuroinflammation. 2024. PMID: 38678300 Free PMC article.
-
Astrocyte-microglia crosstalk in subarachnoid hemorrhage: mechanisms and treatments.Front Immunol. 2025 Jun 30;16:1547858. doi: 10.3389/fimmu.2025.1547858. eCollection 2025. Front Immunol. 2025. PMID: 40661949 Free PMC article. Review.
-
Uncovering SPP1+ Macrophage, Neutrophils and Their Related Diagnostic Biomarkers in Intracranial Aneurysm and Subarachnoid Hemorrhage.J Inflamm Res. 2024 Nov 9;17:8569-8587. doi: 10.2147/JIR.S493828. eCollection 2024. J Inflamm Res. 2024. PMID: 39539729 Free PMC article.
References
-
- Geraghty JR, Davis JL, Testai FD. Neuroinflammation and Microvascular Dysfunction After Experimental Subarachnoid Hemorrhage: Emerging Components of Early Brain Injury Related to Outcome. Neurocritical care. 2019;31(2):373–89. Epub 2019/04/24. doi: 10.1007/s12028-019-00710-x ; PubMed Central PMCID: PMC6759381. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
