

Longitudinal uric acid has nonlinear association with kidney failure and mortality in chronic kidney disease
- PMID: 36894586
- PMCID: PMC9998636
- DOI: 10.1038/s41598-023-30902-7
Longitudinal uric acid has nonlinear association with kidney failure and mortality in chronic kidney disease
Abstract
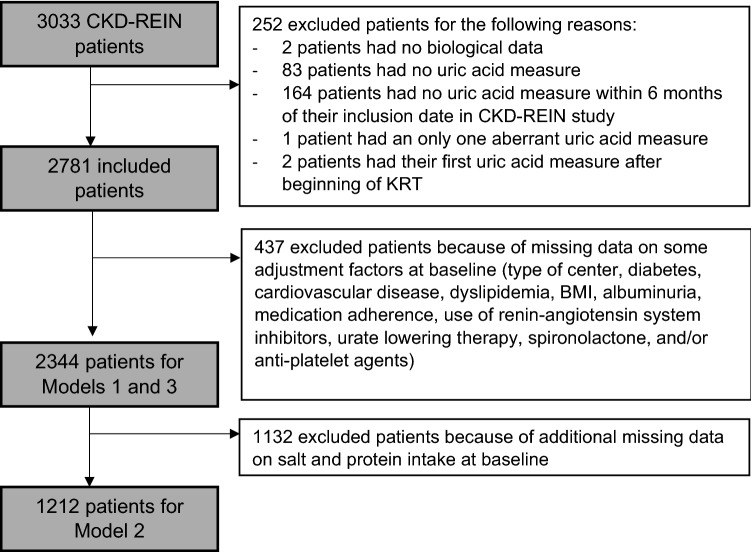
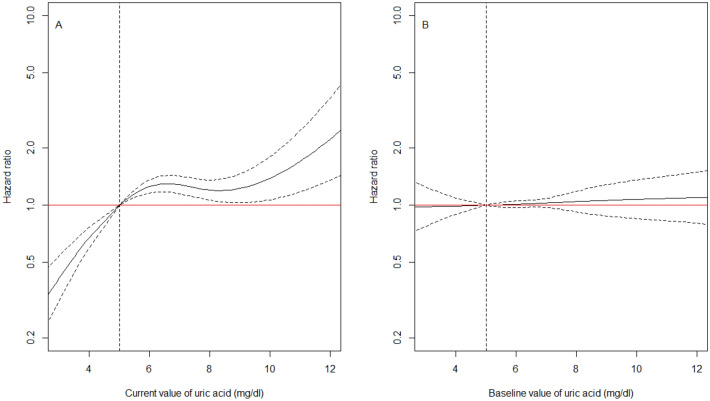
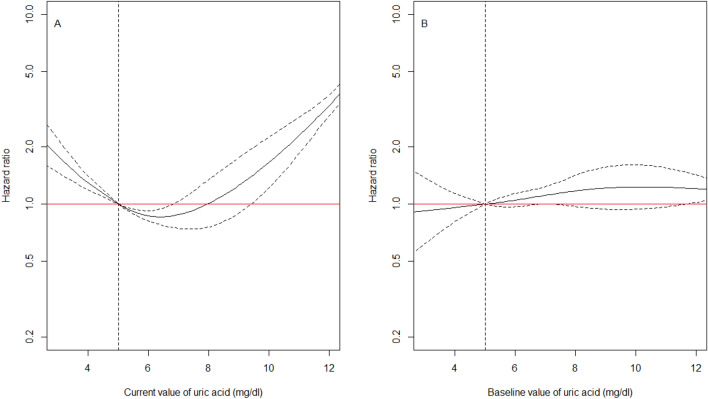
We investigated the shape of the relationship between longitudinal uric acid (UA) and the hazard of kidney failure and death in chronic kidney disease (CKD) patients, and attempted to identify thresholds associated with increased hazards. We included CKD stage 3-5 patients from the CKD-REIN cohort with one serum UA measurement at cohort entry. We used cause-specific multivariate Cox models including a spline function of current values of UA (cUA), estimated from a separate linear mixed model. We followed 2781 patients (66% men, median age, 69 years) for a median of 3.2 years with a median of five longitudinal UA measures per patient. The hazard of kidney failure increased with increasing cUA, with a plateau between 6 and 10 mg/dl and a sharp increase above 11 mg/dl. The hazard of death had a U-shape relationship with cUA, with a hazard twice higher for 3 or 11 mg/dl, compared to 5 mg/dl. In CKD patients, our results indicate that UA above 10 mg/dl is a strong risk marker for kidney failure and death and that low UA levels below 5 mg/dl are associated with death before kidney failure.
© 2023. The Author(s).
Conflict of interest statement
CKD-REIN is supported by a public–private partnership with funding from seven pharmaceutical companies as listed above. The partners did not participate in this work nor in the writing of the manuscript. CKD-REIN is funded by the ‘Agence Nationale de la Recherche’ through the 2010 ‘Cohortes-Investissements d’Avenir’ programme and by the 2010 national ‘Programme Hospitalier de Recherche Clinique’. CKD-REIN is also supported through a public–private partnership with Amgen, Baxter, Fresenius Medical Care, GlaxoSmithKline (GSK), Merck Sharp & Dohme-Chibret (MSD France) since 2012, Lilly France since 2013, Otsuka Pharmaceutical since 2015 and Sanofi-Genzyme from 2012 to 2015. Inserm Transfert set up and has managed this partnership since 2011. The remaining authors do not have any conflict of interest to declare.
Figures
References
-
- Modification of Diet in Renal Disease Study Group, Hunsicker LG, Adler S, Caggiula A, England BK, Greene T, et al. Predictors of the progression of renal disease in the Modification of Diet in Renal Disease Study. Kidney Int.51(6), 1908–1919 (1997). - PubMed
-
- Sturm G, Kollerits B, Neyer U, Ritz E, Kronenberg F, MMKD Study Group. Uric acid as a risk factor for progression of non-diabetic chronic kidney disease? The mild to Moderate Kidney Disease (MMKD) Study. Exp. Gerontol.43(4), 347–352 (2008). - PubMed
-
- Nacak H, van Diepen M, Qureshi AR, Carrero JJ, Stijnen T, Dekker FW, et al. Uric acid is not associated with decline in renal function or time to renal replacement therapy initiation in a referred cohort of patients with Stage III, IV and V chronic kidney disease. Nephrol. Dial. Transpl. 2015;30(12):2039–2045. doi: 10.1093/ndt/gfv225. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
