

Molecular and network-level mechanisms explaining individual differences in autism spectrum disorder
- PMID: 36894656
- PMCID: PMC11446249
- DOI: 10.1038/s41593-023-01259-x
Molecular and network-level mechanisms explaining individual differences in autism spectrum disorder
Abstract
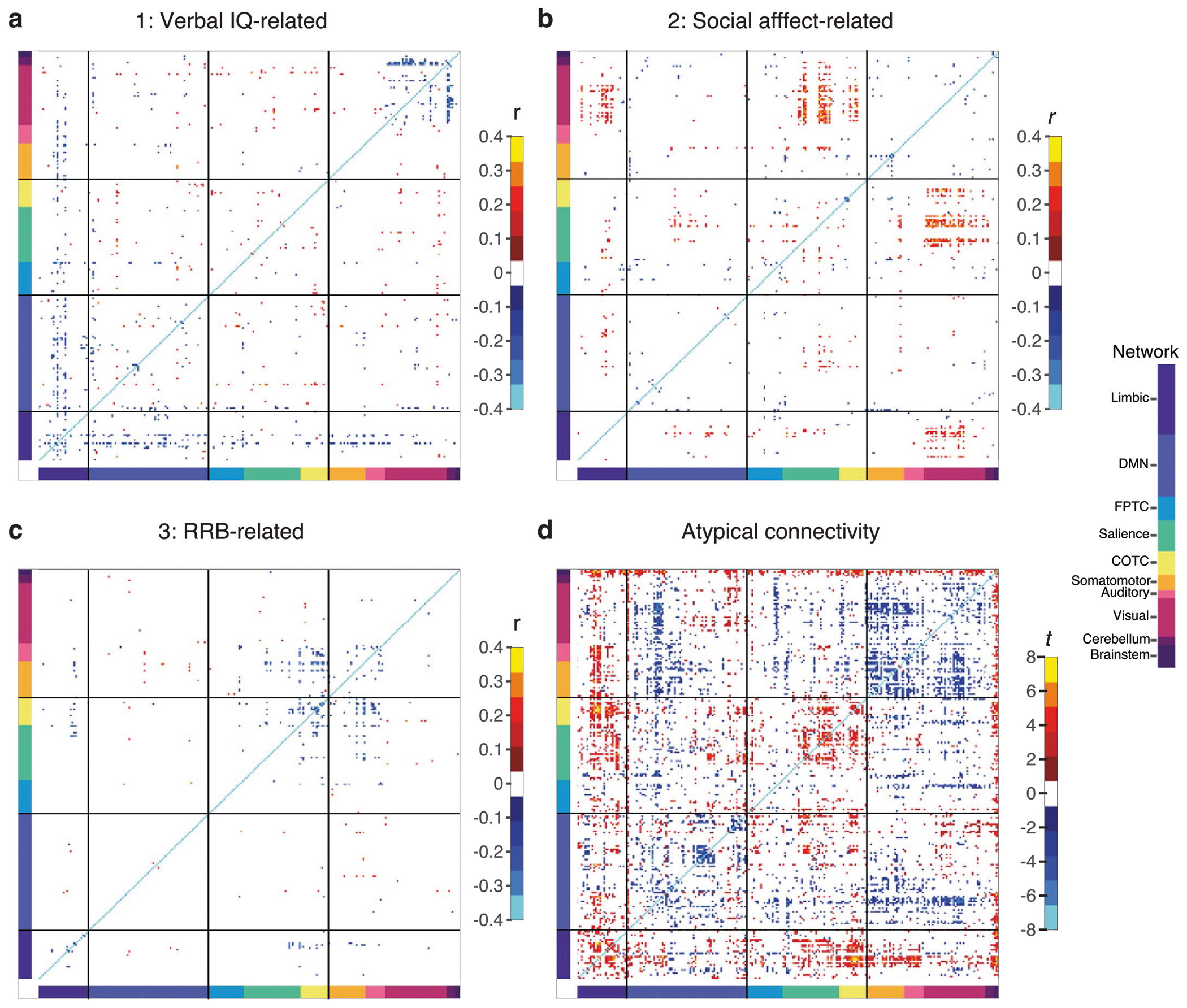
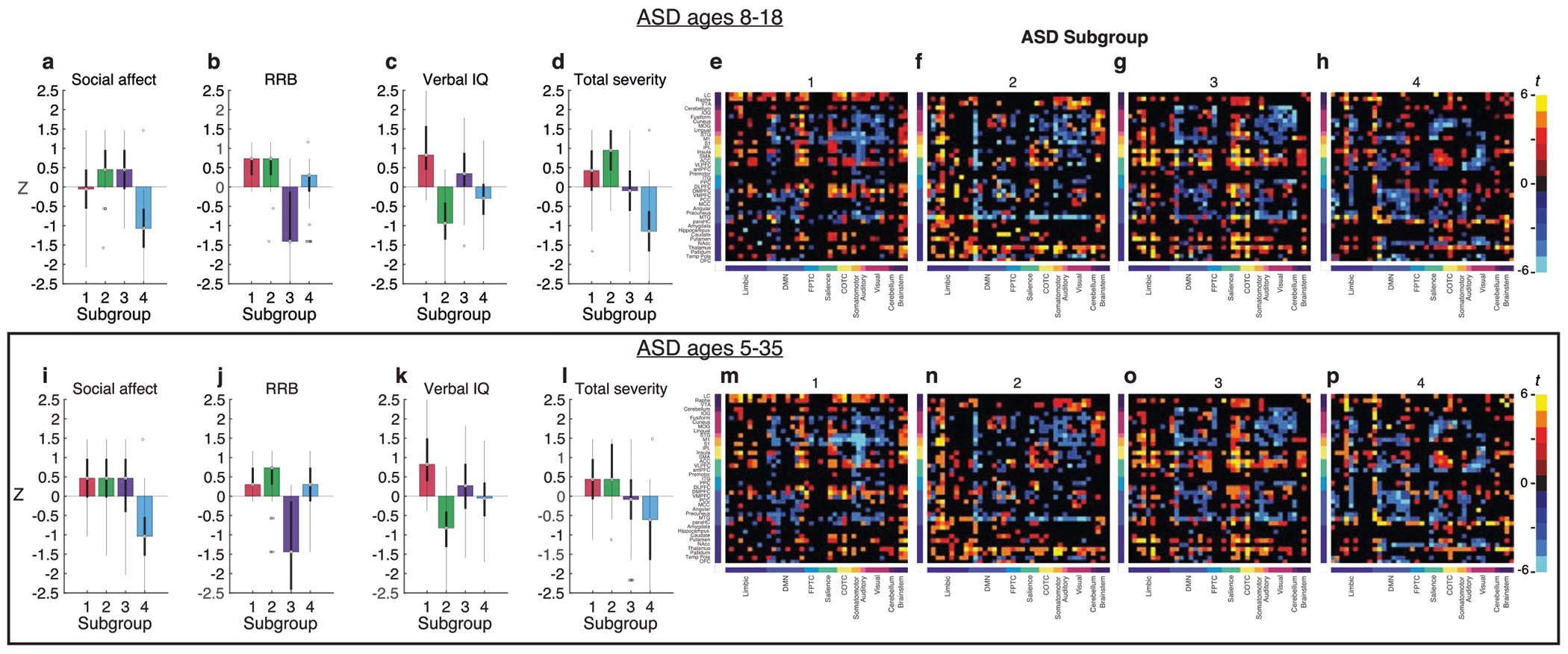
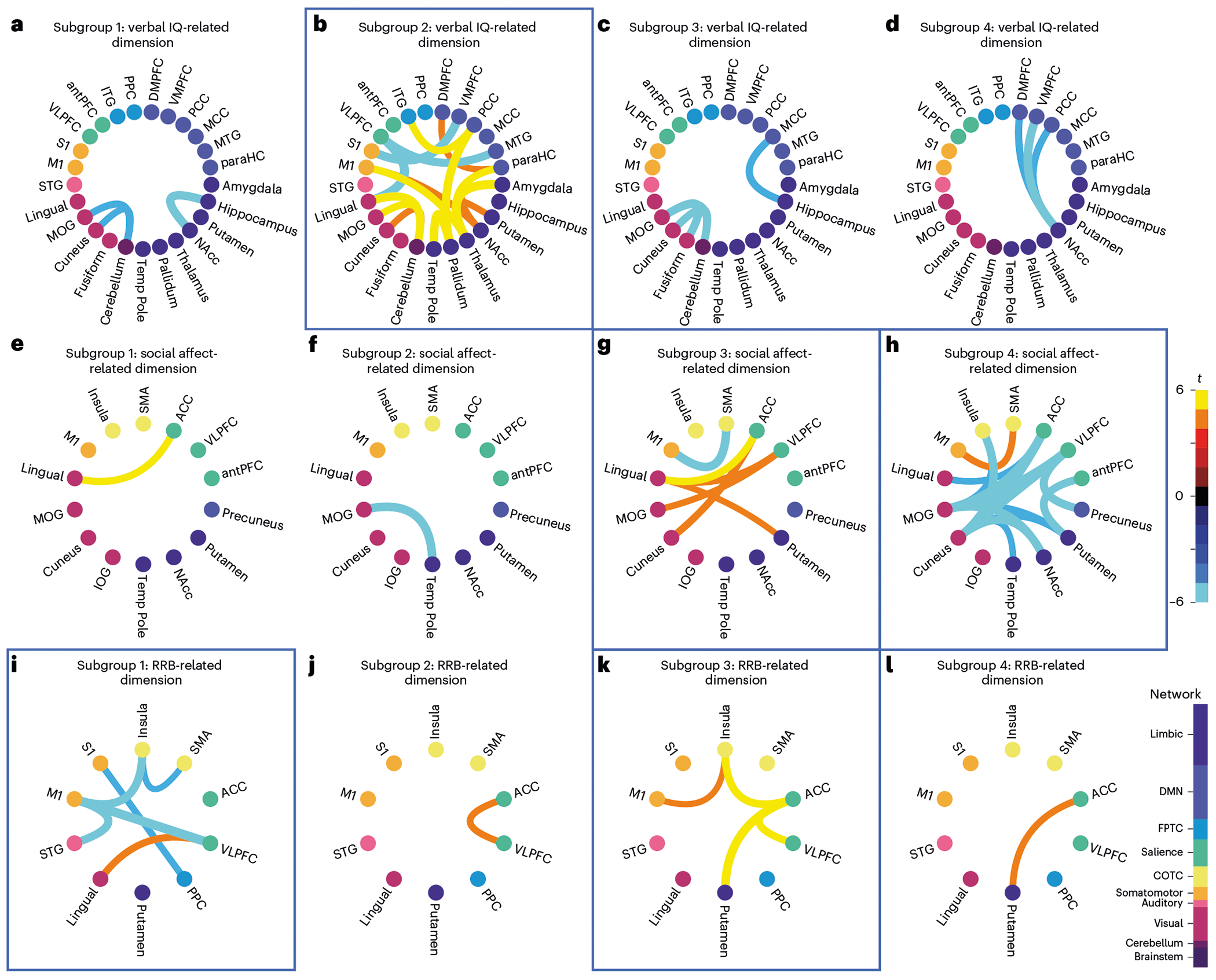
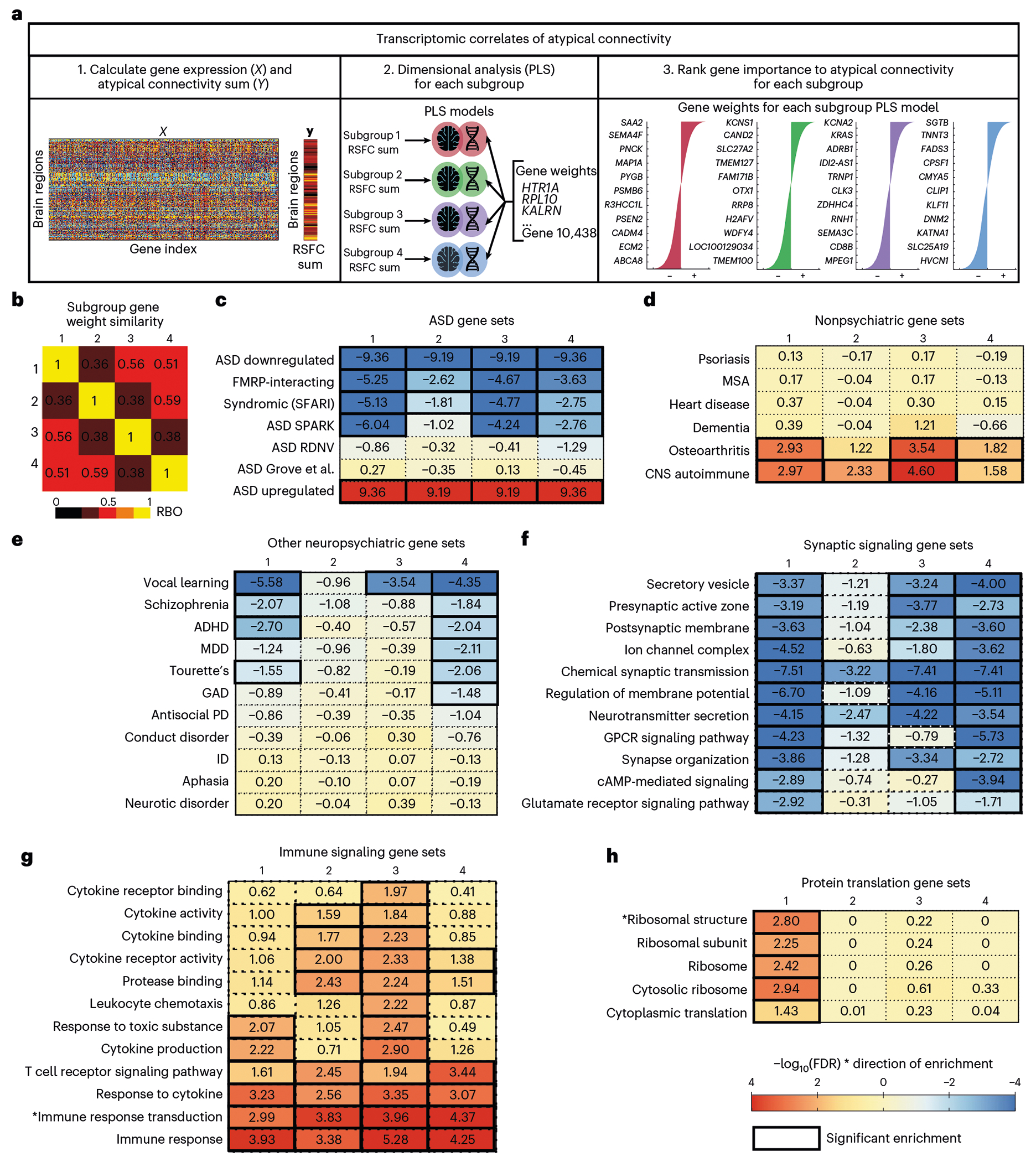
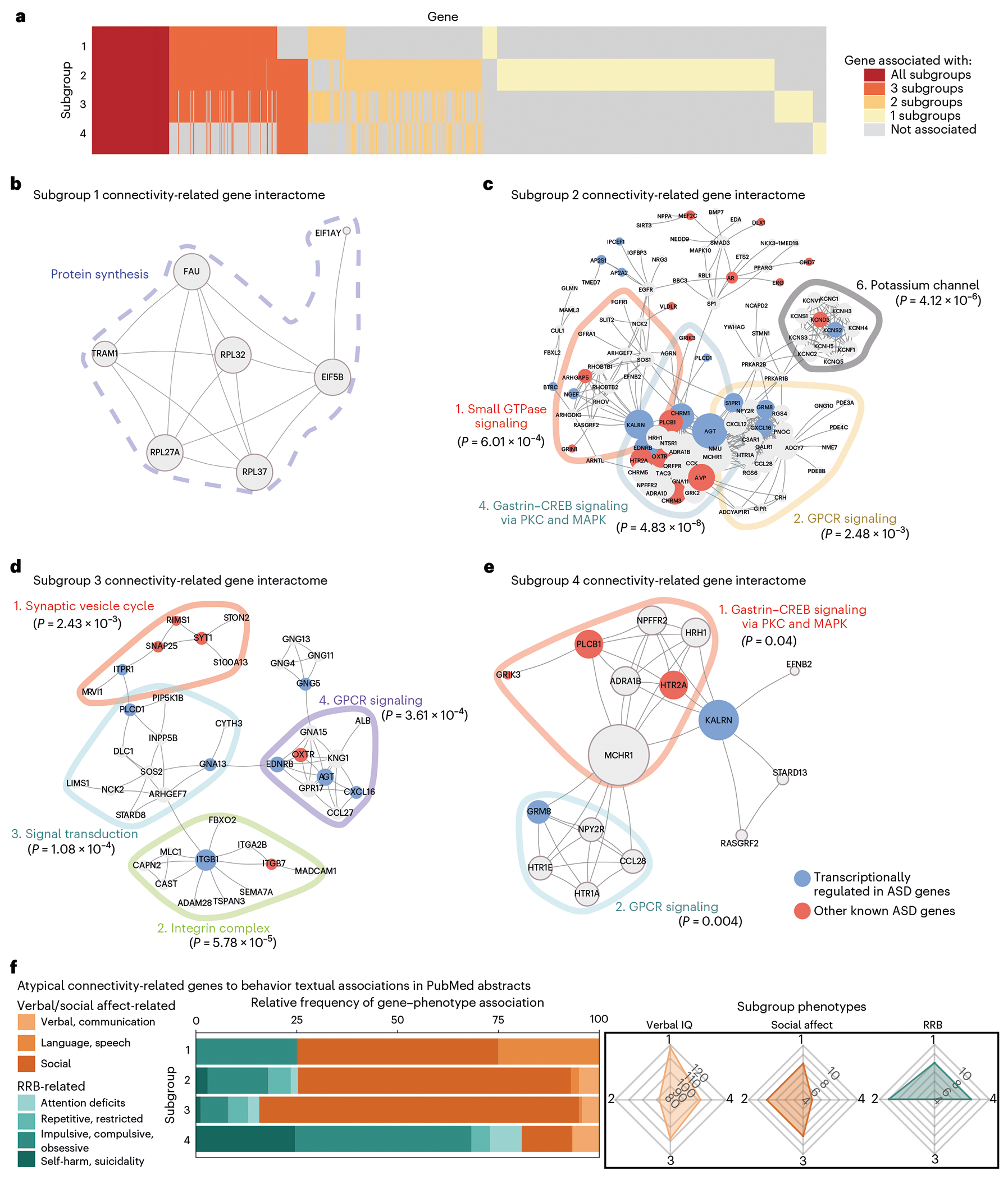
The mechanisms underlying phenotypic heterogeneity in autism spectrum disorder (ASD) are not well understood. Using a large neuroimaging dataset, we identified three latent dimensions of functional brain network connectivity that predicted individual differences in ASD behaviors and were stable in cross-validation. Clustering along these three dimensions revealed four reproducible ASD subgroups with distinct functional connectivity alterations in ASD-related networks and clinical symptom profiles that were reproducible in an independent sample. By integrating neuroimaging data with normative gene expression data from two independent transcriptomic atlases, we found that within each subgroup, ASD-related functional connectivity was explained by regional differences in the expression of distinct ASD-related gene sets. These gene sets were differentially associated with distinct molecular signaling pathways involving immune and synapse function, G-protein-coupled receptor signaling, protein synthesis and other processes. Collectively, our findings delineate atypical connectivity patterns underlying different forms of ASD that implicate distinct molecular signaling mechanisms.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Competing interests
C.L. is listed as an inventor for Cornell University patent applications on neuroimaging biomarkers for depression that are pending or in preparation. C.L. has served as a scientific advisor or consultant to Compass Pathways, Delix Therapeutics, Magnus Medical and Brainify. AI. The authors declare no other competing interests.
Figures











References
-
- Insel T. et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am. J. Psychiatry 167, 748–751 (2010). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
