

Proton beam therapy for cervical lymph node metastasis in an octogenarian with melanoma of unknown primary: a case report
- PMID: 36896196
- PMCID: PMC9989079
- DOI: 10.1007/s13691-023-00597-8
Proton beam therapy for cervical lymph node metastasis in an octogenarian with melanoma of unknown primary: a case report
Abstract
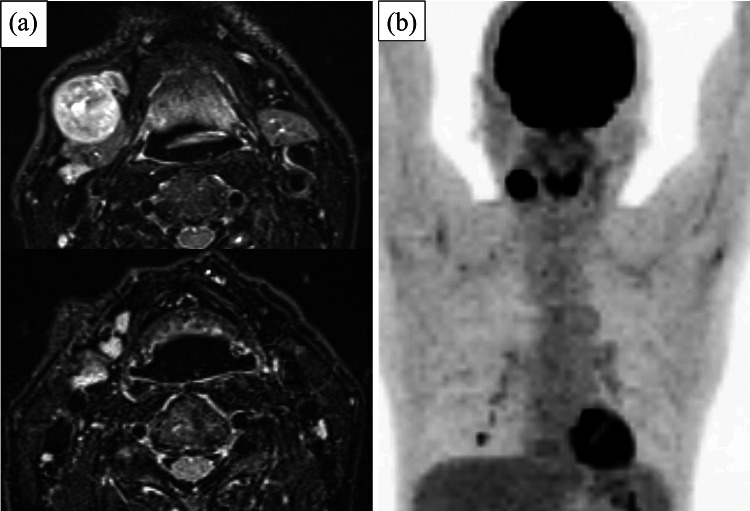
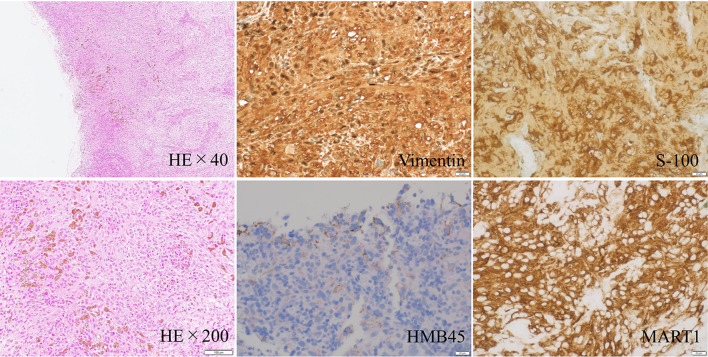
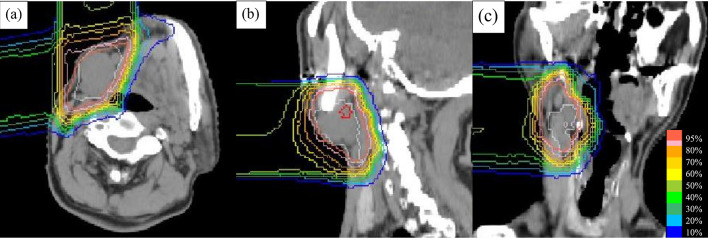
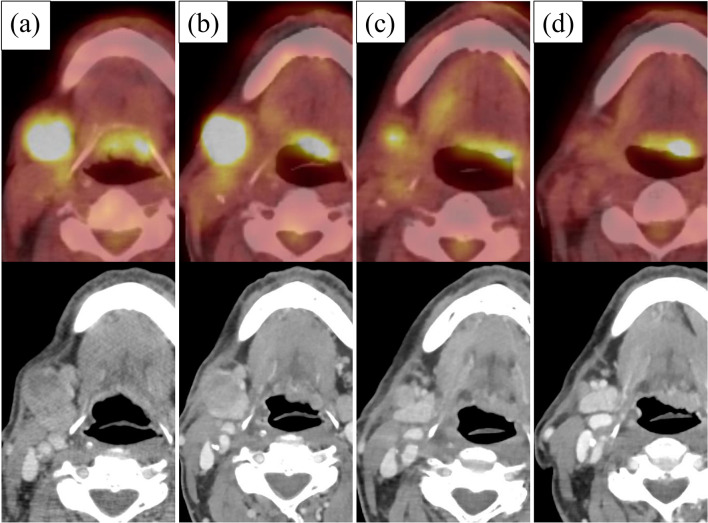
An 80-year-old man with an approximately 3-cm mass in the right submandibular region presented to our institution. Magnetic resonance imaging revealed enlarged lymph nodes (LNs) in the right neck, and fluorine-18-2-deoxy-D-glucose (FDG) positron emission tomography (PET)/computed tomography (CT) indicated positive FDG accumulation in the right neck LNs only. Excisional biopsy was performed for suspected malignant lymphoma, and the biopsy revealed melanoma. Close examination of the skin, nasal cavity, oral pharyngeal and laryngeal cavities, and gastrointestinal tract were performed. No primary tumor was detected by these examinations, and the patient was diagnosed with cervical LN metastasis from melanoma of unknown primary of clinical stage T0N3bM0 stage IIIC. The patient refused cervical neck dissection because of his age and comorbidity of Alzheimer's disease and instead opted for proton beam therapy (PBT) at a total dose of 69 Gy (relative biological effectiveness) in 23 fractions. He did not receive any systemic therapy. The enlarged LNs shrunk slowly, and FDG PET/CT at 1 year after PBT showed that the right submandibular LN had shrunk from 27 to 7 mm in length, and there was no significant FDG accumulation. At 6 years and 4 months after PBT, the patient is alive without any recurrence.
Keywords: Lymph node metastasis; Melanoma of unknown primary; Proton beam therapy.
© The Author(s) 2023.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflicts of interest regarding this manuscript.
Figures
Similar articles
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Preliminary report of using FDG-PET to detect extrapelvic lesions in cervical cancer patients with enlarged pelvic lymph nodes on MRI/CT.Int J Radiat Oncol Biol Phys. 2004 Apr 1;58(5):1506-12. doi: 10.1016/j.ijrobp.2003.09.013. Int J Radiat Oncol Biol Phys. 2004. PMID: 15050330
-
Prognostic value of (18)F-fluorodeoxyglucose positron emission tomography, computed tomography and magnetic resonance imaging in oral cavity squamous cell carcinoma with pathologically positive neck lymph node.Radiat Oncol J. 2012 Dec;30(4):173-81. doi: 10.3857/roj.2012.30.4.173. Epub 2012 Dec 31. Radiat Oncol J. 2012. PMID: 23346536 Free PMC article.
-
Cervical metastasis of gingival carcinoma misdiagnosed as branchiogenic carcinoma, a rare entity - report of a case and review of literature.BMC Oral Health. 2017 Nov 28;17(1):139. doi: 10.1186/s12903-017-0435-9. BMC Oral Health. 2017. PMID: 29183323 Free PMC article. Review.
-
Diagnostic accuracy of F-18 FDG PET or PET/CT for detection of lymph node metastasis in clinically node negative head and neck cancer patients; A systematic review and meta-analysis.Am J Otolaryngol. 2019 Mar-Apr;40(2):297-305. doi: 10.1016/j.amjoto.2018.10.013. Epub 2018 Oct 23. Am J Otolaryngol. 2019. PMID: 30473166
Cited by
-
Comprehensive Literature Review on Melanoma of Unknown Primary Site Triggered by an Intriguing Case Report.Diagnostics (Basel). 2024 Oct 3;14(19):2210. doi: 10.3390/diagnostics14192210. Diagnostics (Basel). 2024. PMID: 39410614 Free PMC article.
References
-
- Dasgupta T, Bowden L, Berg JW. Malignant melanoma of unknown primary origin. Surg Gynecol Obstet. 1963;117:341–345. - PubMed
Publication types
LinkOut - more resources
Full Text Sources