

Genetically determined cardiomyopathies at autopsy: the pivotal role of the pathologist in establishing the diagnosis and guiding family screening
- PMID: 36897369
- PMCID: PMC10067659
- DOI: 10.1007/s00428-023-03523-8
Genetically determined cardiomyopathies at autopsy: the pivotal role of the pathologist in establishing the diagnosis and guiding family screening
Abstract
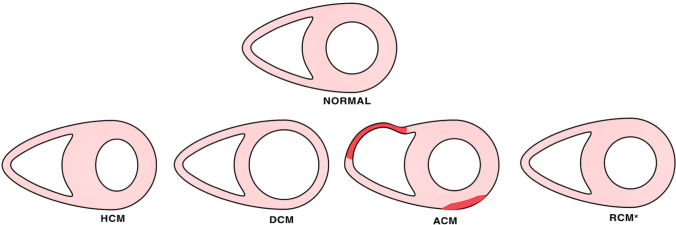
Cardiomyopathies (CMP) comprise a heterogenous group of diseases affecting primarily the myocardium, either genetic and/or acquired in origin. While many classification systems have been proposed in the clinical setting, there is no internationally agreed pathological consensus concerning the diagnostic approach to inherited CMP at autopsy. A document on autopsy diagnosis of CMP is needed because the complexity of the pathologic backgrounds requires proper insight and expertise. In cases presenting with cardiac hypertrophy and/or dilatation/scarring with normal coronary arteries, a suspicion of inherited CMP must be considered, and a histological examination is essential. Establishing the actual cause of the disease may require a number of tissue-based and/or fluid-based investigations, be it histological, ultrastructural, or molecular. A history of illicit drug use must be looked for. Sudden death is frequently the first manifestation of disease in case of CMP, especially in the young. Also, during routine clinical or forensic autopsies, a suspicion of CMP may arise based on clinical data or pathological findings at autopsy. It is thus a challenge to make a diagnosis of a CMP at autopsy. The pathology report should provide the relevant data and a cardiac diagnosis which can help the family in furthering investigations, including genetic testing in case of genetic forms of CMP. With the explosion in molecular testing and the concept of the molecular autopsy, the pathologist should use strict criteria in the diagnosis of CMP, and helpful for clinical geneticists and cardiologists who advise the family as to the possibility of a genetic disease.
Keywords: Autopsy; Cardiomyopathies; Genetic; Sudden cardiac death.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Challenges of genetics in the diagnosis of sudden cardiac death. Interest for forensic and legal medicine.Med Clin (Barc). 2025 Feb 14;164(3):e1-e7. doi: 10.1016/j.medcli.2024.10.002. Epub 2024 Nov 18. Med Clin (Barc). 2025. PMID: 39562230 Review. English, Spanish.
-
Histopathological diagnosis of arrhythmogenic right ventricular cardiomyopathy: A review of three autopsy cases.Malays J Pathol. 2022 Aug;44(2):277-283. Malays J Pathol. 2022. PMID: 36043591 Review.
-
Genetic analysis of sudden cardiac death victims: a survey of current forensic autopsy practices.Int J Legal Med. 2011 May;125(3):359-66. doi: 10.1007/s00414-010-0474-0. Epub 2010 Jun 11. Int J Legal Med. 2011. PMID: 20535491
-
[Molecular autopsy of sudden cardiac death: from postmortem to clinical approach].Rev Med Suisse. 2008 Jul 2;4(164):1590-3. Rev Med Suisse. 2008. PMID: 18711970 French.
-
Is there progress in the autopsy diagnosis of sudden unexpected death in adults?Forensic Sci Int. 2006 Jan 27;156(2-3):138-44. doi: 10.1016/j.forsciint.2004.12.024. Forensic Sci Int. 2006. PMID: 16410164 Review.
Cited by
-
Autopsy of all young sudden death cases is important to increase survival in family members left behind.Europace. 2024 Jun 3;26(6):euae128. doi: 10.1093/europace/euae128. Europace. 2024. PMID: 38715537 Free PMC article. Review.
-
The Role of miRNA Expression Profile in Sudden Cardiac Death Cases.Genes (Basel). 2023 Oct 17;14(10):1954. doi: 10.3390/genes14101954. Genes (Basel). 2023. PMID: 37895303 Free PMC article. Review.
-
Ischemic and non-ischemic myocardial injuries at autopsy- an overview for forensic pathologists.Int J Legal Med. 2025 Jul;139(4):1579-1596. doi: 10.1007/s00414-025-03479-1. Epub 2025 Apr 2. Int J Legal Med. 2025. PMID: 40172635 Free PMC article. Review.
-
Concealed cardiomyopathy as an emerging cause of sudden cardiac arrest and sudden cardiac death.Nat Cardiovasc Res. 2024 Nov;3(11):1274-1283. doi: 10.1038/s44161-024-00558-1. Epub 2024 Nov 1. Nat Cardiovasc Res. 2024. PMID: 39487366 Review.
-
RBM20 p.Arg636Cys: A Pathogenic Variant Identified in a Family with Several Cases of Unexpected Sudden Deaths.J Clin Med. 2025 Jan 24;14(3):743. doi: 10.3390/jcm14030743. J Clin Med. 2025. PMID: 39941414 Free PMC article.
References
-
- Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O'Connell J, Olsen E, Thiene G, Goodwin J, Gyarfas I, Martin I, Nordet P. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation. 1996;93:841–842. doi: 10.1161/01.cir.93.5.841. - DOI - PubMed
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB, American Heart A Council on Clinical Cardiology HF Transplantation C Quality of C Outcomes R Functional G Translational Biology Interdisciplinary Working G Council on E Prevention Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. doi: 10.1161/CIRCULATIONAHA.106.174287. - DOI - PubMed
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, Dubourg O, Kuhl U, Maisch B, McKenna WJ, Monserrat L, Pankuweit S, Rapezzi C, Seferovic P, Tavazzi L, Keren A. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–276. doi: 10.1093/eurheartj/ehm342. - DOI - PubMed
-
- Arbustini E, Narula N, Dec GW, Reddy KS, Greenberg B, Kushwaha S, Marwick T, Pinney S, Bellazzi R, Favalli V, Kramer C, Roberts R, Zoghbi WA, Bonow R, Tavazzi L, Fuster V, Narula J. The MOGE(S) classification for a phenotype-genotype nomenclature of cardiomyopathy: endorsed by the World Heart Federation. J Am Coll Cardiol. 2013;62:2046–2072. doi: 10.1016/j.jacc.2013.08.1644. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
