

Tailoring the optimal duration of the extended adjuvant endocrine therapy in patients with early-stage breast cancer. A systematic review and meta-analysis of randomized clinical trials
- PMID: 36898259
- PMCID: PMC10020092
- DOI: 10.1016/j.breast.2023.02.012
Tailoring the optimal duration of the extended adjuvant endocrine therapy in patients with early-stage breast cancer. A systematic review and meta-analysis of randomized clinical trials
Abstract
Background: Controversy exists regarding the optimal duration of the extended adjuvant endocrine treatment (ET) in patients with early-stage breast-cancer (eBC). We performed a systematic review and trial-level meta-analysis of all randomized clinical trials (RCTs) comparing a "limited-extended" adjuvant ET (defined as more than 5 but less than 7.5 years of treatment overall) versus a "full-extended" adjuvant ET (defined as more than 7.5 years of treatment overall) in eBC.
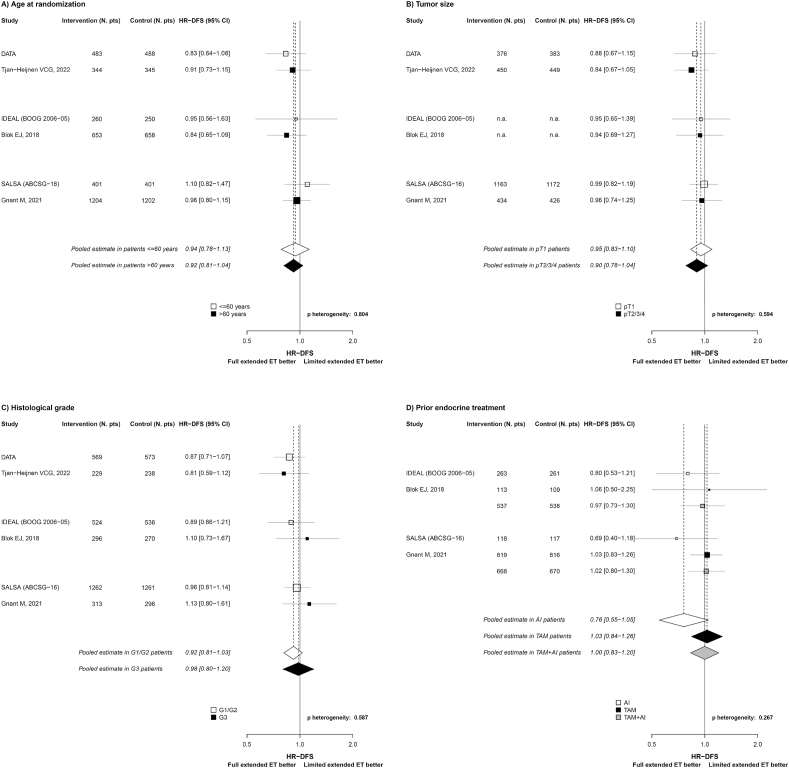
Methods: To be eligible, RCTs had to i) compare a "limited-extended" adjuvant ET versus a "full-extended" adjuvant ET in patients with eBC; and ii) report disease-free survival (DFS) hazard ratio (HR) according to the disease nodal-status [i.e., nodal-negative (N-ve) versus nodal-positive (N + ve)]. The primary endpoint was to assess the difference in efficacy of full-versus limited-extended ET, measured in terms of the difference in DFS log-HR, according to the disease nodal-status. Secondary endpoint was the difference in efficacy of full-versus limited-extended ET according to tumor size (i.e., pT1 vs pT2/3/4), histological grade (i.e., G1/G2 vs G3), patients' age (i.e., ≤60 vs > 60 years) and previous type of ET (i.e., aromatase inhibitors vs tamoxifen vs switch strategy).
Results: Three phase III RCTs fulfilled the inclusion criteria. A total of 6689 patients were included in the analysis, of which 3506 (53%) had N + ve disease. The full-extended ET provided no DFS-benefit as compared with the limited-extended ET in patients with N-ve disease (pooled DFS-HR = 1.04, 95%CI: 0.89 to 1.22; I2 = 18%). Conversely, in patients with N + ve disease the full-extended ET significantly improved DFS, with a pooled DFS-HR of 0.85 (95%CI: 0.74 to 0.97; I2 = 0%). There was a significant interaction between the disease nodal-status and the efficacy of the full-versus limited-extended ET (p-heterogeneity = 0.048). The full-extended ET provided no significant DFS-benefit as compared with the limited-extended ET in all the other subgroups analyzed.
Conclusions: Patients with eBC and N + ve disease can obtain a significant DFS-benefit from the full-extended as compared with the limited-extended adjuvant ET.
Keywords: Disease nodal status; Early breast cancer; Extended adjuvant endocrine therapy; meta-analysis.
Copyright © 2023. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of competing interest All other authors declare no conflicts of interest. The lead author (FC) affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Figures


References
-
- Burstein H.J., Lacchetti C., Anderson H., Buchholz T.A., Davidson N.E., Gelmon K.A., et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J Clin Oncol. 2019;37(5):423–438. - PubMed
-
- Davies C., Pan H., Godwin J., Gray R., Arriagada R., Raina V., et al. Adjuvant Tamoxifen: longer against Shorter (ATLAS) Collaborative Group. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381(9869):805–816. - PMC - PubMed
-
- Goss P.E., Ingle J.N., Martino S., Robert N.J., Muss H.B., Piccart M.J., et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med. 2003;349(19):1793–1802. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
