

Phase 2 Trial of Stereotactic Ablative Radiotherapy for Patients with Primary Renal Cancer
- PMID: 36898872
- PMCID: PMC10440291
- DOI: 10.1016/j.eururo.2023.02.016
Phase 2 Trial of Stereotactic Ablative Radiotherapy for Patients with Primary Renal Cancer
Abstract
Background: Most renal cell carcinomas (RCCs) are localized and managed by active surveillance, surgery, or minimally invasive techniques. Stereotactic ablative radiation (SAbR) may provide an innovative non-invasive alternative although prospective data are limited.
Objective: To investigate whether SAbR is effective in the management of primary RCCs.
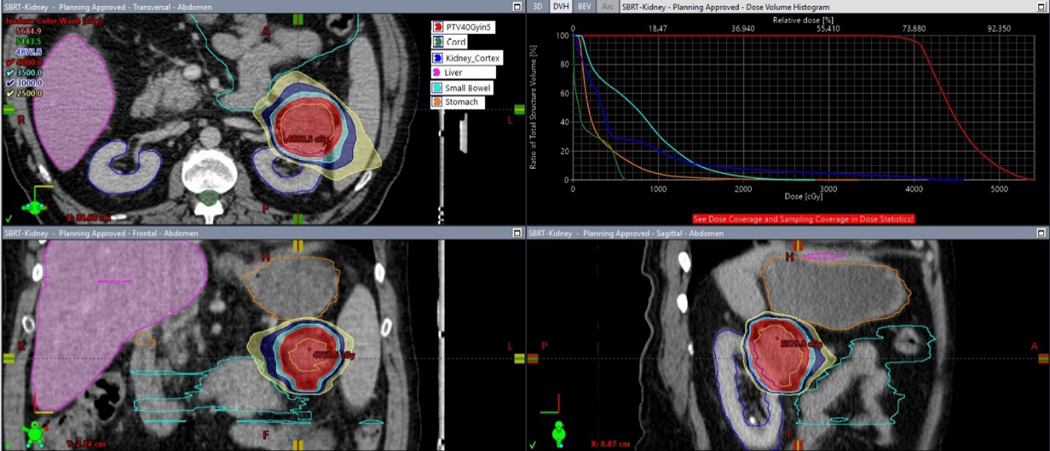
Design, setting, and participants: Patients with biopsy-confirmed radiographically enlarging primary RCC (≤5 cm) were enrolled. SAbR was delivered in either three (12 Gy) or five (8 Gy) fractions.
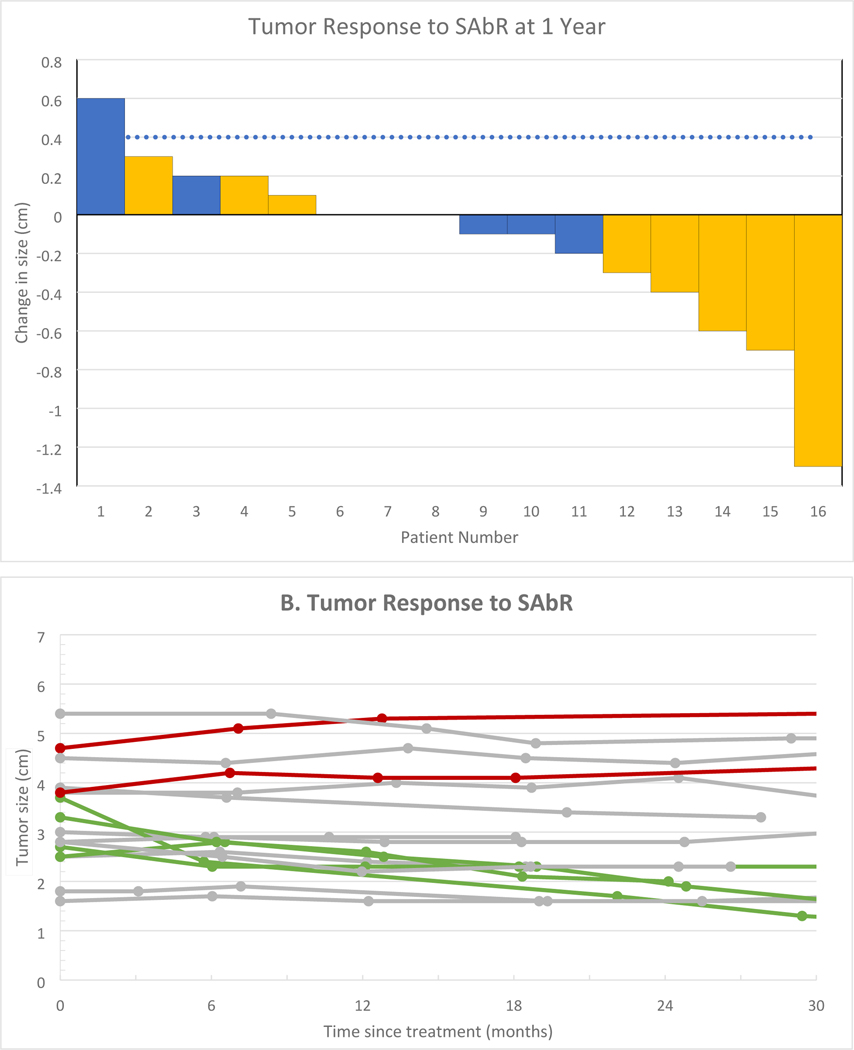
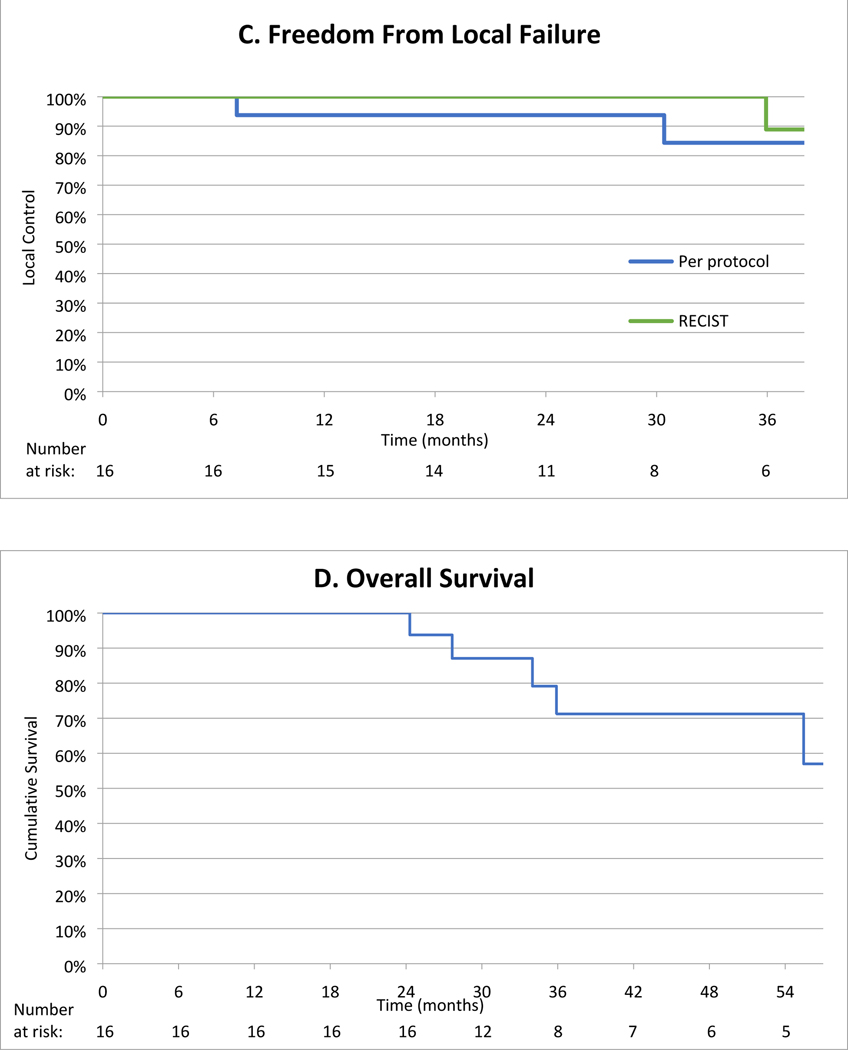
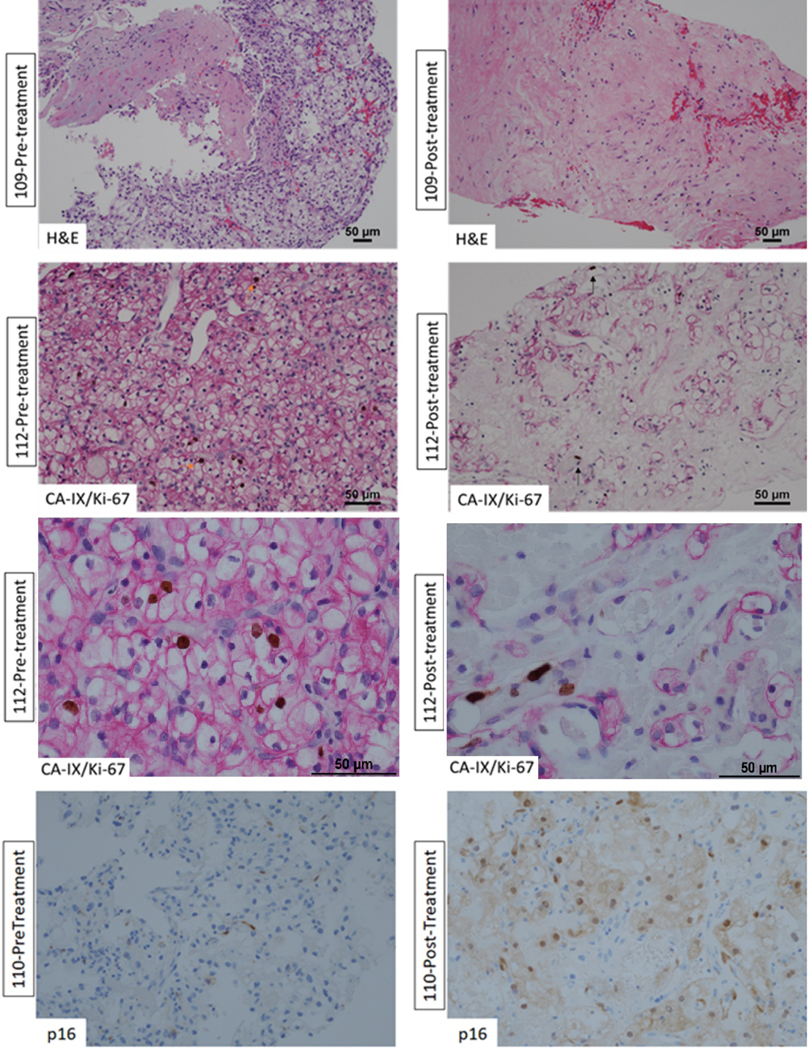
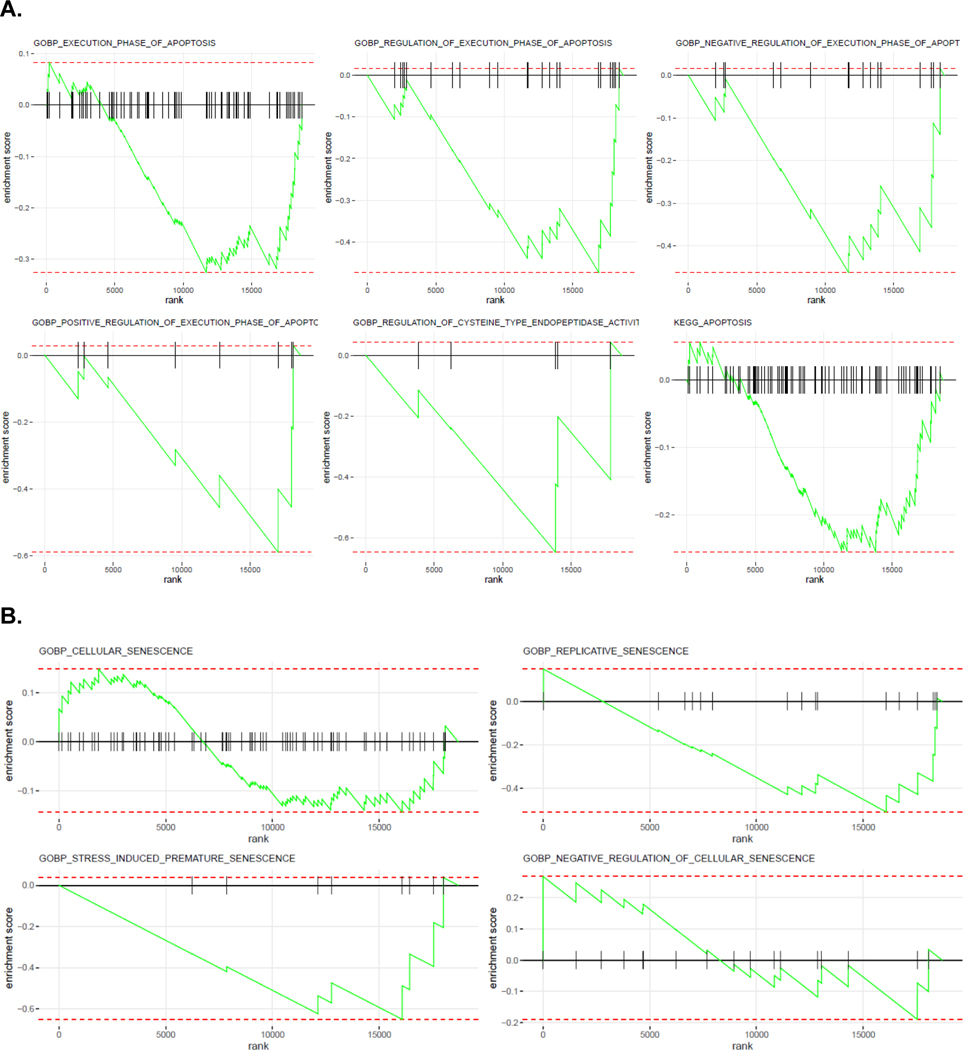
Outcome measurements and statistical analysis: The primary endpoint was local control (LC) defined as a reduction in tumor growth rate (compared with a benchmark of 4 mm/yr on active surveillance) and pathologic evidence of tumor response at 1 yr. Secondary endpoints included LC by the Response Evaluation Criteria in Solid Tumors (RECIST 1.1), safety, and preservation of kidney function. Exploratory tumor cell-enriched spatial protein and gene expression analysis were conducted on pre- and post-treatment biopsy samples.
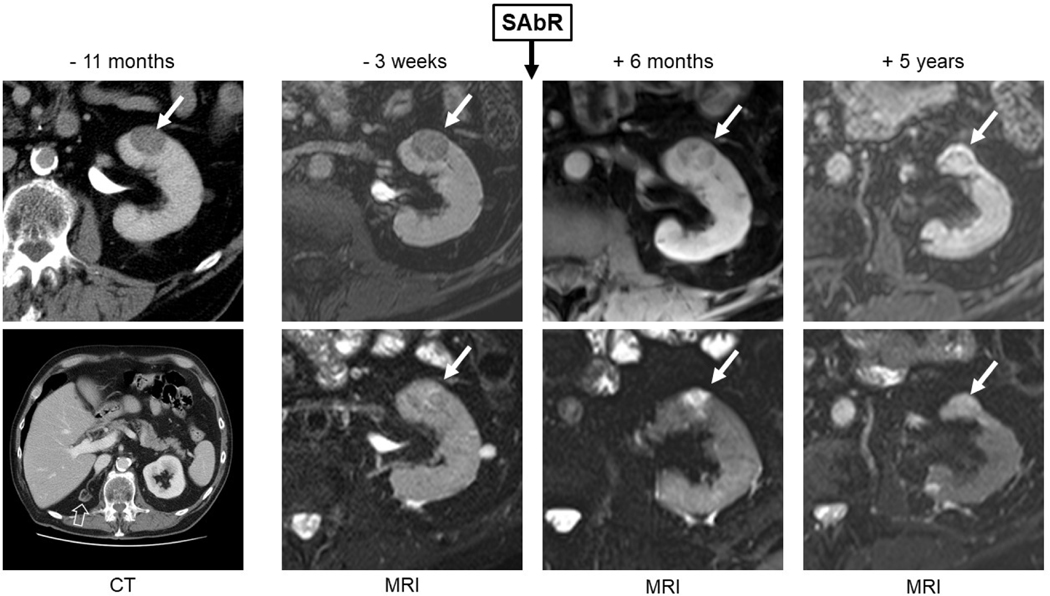
Results and limitations: Target accrual was reached with the enrollment of 16 ethnically diverse patients. Radiographic LC at 1 yr was observed in 94% of patients (15/16; 95% confidence interval: 70, 100), and this was accompanied by pathologic evidence of tumor response (hyalinization, necrosis, and reduced tumor cellularity) in all patients. By RECIST, 100% of the sites remained without progression at 1 yr. The median pretreatment growth rate was 0.8 cm/yr (interquartile range [IQR]: 0.3, 1.4), and the median post-treatment growth rate was 0.0 cm/yr (IQR: -0.4, 0.1, p < 0.002). Tumor cell viability decreased from 4.6% to 0.7% at 1 yr (p = 0.004). With a median follow-up of 36 mo for censored patients, the disease control rate was 94%. SAbR was well tolerated with no grade ≥2 (acute or late) toxicities. The average glomerular filtration rate declined from a baseline of 65.6 to 55.4 ml/min at 1 yr (p = 0.003). Spatial protein and gene expression analyses were consistent with the induction of cellular senescence by radiation.
Conclusions: This clinical trial adds to the growing body of evidence suggesting that SAbR is effective for primary RCC supporting its evaluation in comparative phase 3 clinical trials.
Patient summary: In this clinical trial, we investigated a noninvasive treatment option of stereotactic radiation therapy for the treatment of primary kidney cancer and found that it was safe and effective.
Keywords: Primary renal cell carcinoma; Renal cell carcinoma; Senescence; Stereotactic ablative radiotherapy.
Copyright © 2023 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Stereotactic Radiotherapy for Renal Cell Carcinoma: The Fallacy of (False) Positive Post-treatment Biopsy?Eur Urol. 2023 Sep;84(3):287-288. doi: 10.1016/j.eururo.2023.03.025. Epub 2023 Apr 7. Eur Urol. 2023. PMID: 37032187 No abstract available.
-
Stereotactic ablative radiotherapy: a game-changer in primary renal cancer therapy.Transl Androl Urol. 2024 Jul 31;13(7):1312-1314. doi: 10.21037/tau-23-663. Epub 2024 Jul 16. Transl Androl Urol. 2024. PMID: 39100826 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7–33. - PubMed
-
- Jayson M, Sanders H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology 1998;51:203–5. - PubMed
-
- Smith SJ, Bosniak MA, Megibow AJ, Hulnick DH, Horii SC, Raghavendra BN. Renal cell carcinoma: earlier discovery and increased detection. Radiology 1989;170(3 Pt 1):699–703. - PubMed
-
- Howlader N, Noone AM, Krapcho M, et al. , editors. SEER cancer statistics review, 1975−2017. Bethesda, MD: National Cancer Institute; April 2020. https://seer.cancer.gov/csr/1975_2017/
-
- Fontenil A, Bigot P, Bernhard JC, et al. Who is dying after nephrectomy for cancer? Study of risk factors and causes of death after analyzing morbidity and mortality reviews (UroCCR-33 study). Progr Urol 2019;29:282–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
