

Indoor air surveillance and factors associated with respiratory pathogen detection in community settings in Belgium
- PMID: 36898982
- PMCID: PMC10005919
- DOI: 10.1038/s41467-023-36986-z
Indoor air surveillance and factors associated with respiratory pathogen detection in community settings in Belgium
Abstract
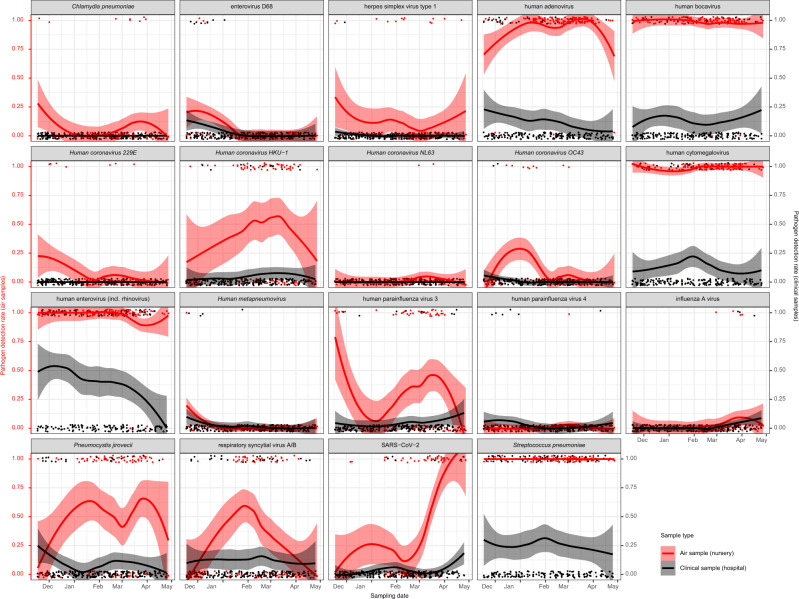
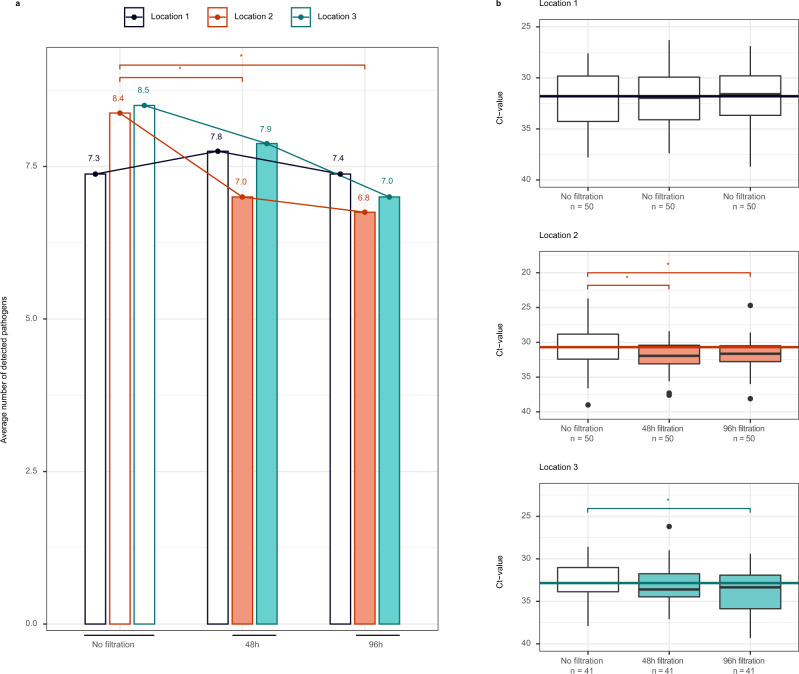
Currently, the real-life impact of indoor climate, human behaviour, ventilation and air filtration on respiratory pathogen detection and concentration are poorly understood. This hinders the interpretability of bioaerosol quantification in indoor air to surveil respiratory pathogens and transmission risk. We tested 341 indoor air samples from 21 community settings in Belgium for 29 respiratory pathogens using qPCR. On average, 3.9 pathogens were positive per sample and 85.3% of samples tested positive for at least one. Pathogen detection and concentration varied significantly by pathogen, month, and age group in generalised linear (mixed) models and generalised estimating equations. High CO2 and low natural ventilation were independent risk factors for detection. The odds ratio for detection was 1.09 (95% CI 1.03-1.15) per 100 parts per million (ppm) increase in CO2, and 0.88 (95% CI 0.80-0.97) per stepwise increase in natural ventilation (on a Likert scale). CO2 concentration and portable air filtration were independently associated with pathogen concentration. Each 100ppm increase in CO2 was associated with a qPCR Ct value decrease of 0.08 (95% CI -0.12 to -0.04), and portable air filtration with a 0.58 (95% CI 0.25-0.91) increase. The effects of occupancy, sampling duration, mask wearing, vocalisation, temperature, humidity and mechanical ventilation were not significant. Our results support the importance of ventilation and air filtration to reduce transmission.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
