

Pathogenesis Underlying Neurological Manifestations of Long COVID Syndrome and Potential Therapeutics
- PMID: 36899952
- PMCID: PMC10001044
- DOI: 10.3390/cells12050816
Pathogenesis Underlying Neurological Manifestations of Long COVID Syndrome and Potential Therapeutics
Abstract
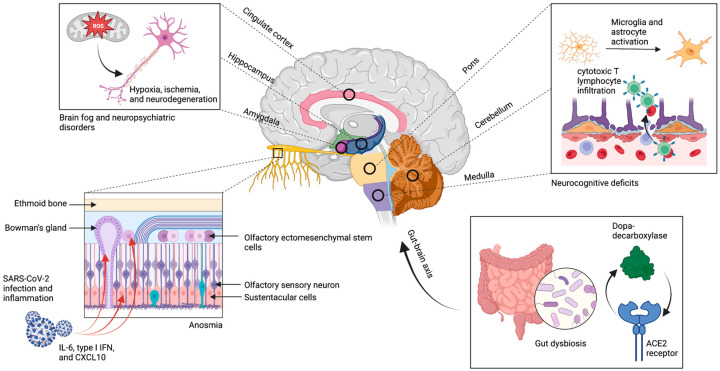
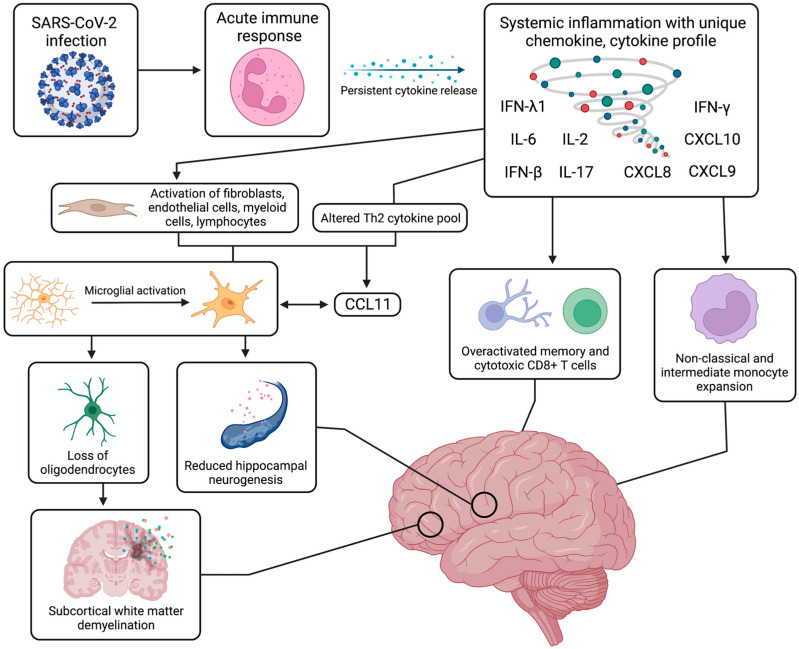
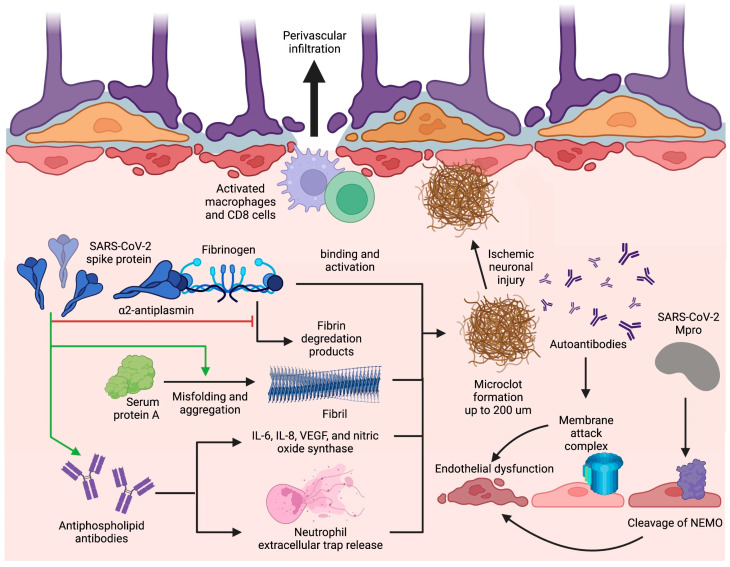
The development of long-term symptoms of coronavirus disease 2019 (COVID-19) more than four weeks after primary infection, termed "long COVID" or post-acute sequela of COVID-19 (PASC), can implicate persistent neurological complications in up to one third of patients and present as fatigue, "brain fog", headaches, cognitive impairment, dysautonomia, neuropsychiatric symptoms, anosmia, hypogeusia, and peripheral neuropathy. Pathogenic mechanisms of these symptoms of long COVID remain largely unclear; however, several hypotheses implicate both nervous system and systemic pathogenic mechanisms such as SARS-CoV2 viral persistence and neuroinvasion, abnormal immunological response, autoimmunity, coagulopathies, and endotheliopathy. Outside of the CNS, SARS-CoV-2 can invade the support and stem cells of the olfactory epithelium leading to persistent alterations to olfactory function. SARS-CoV-2 infection may induce abnormalities in innate and adaptive immunity including monocyte expansion, T-cell exhaustion, and prolonged cytokine release, which may cause neuroinflammatory responses and microglia activation, white matter abnormalities, and microvascular changes. Additionally, microvascular clot formation can occlude capillaries and endotheliopathy, due to SARS-CoV-2 protease activity and complement activation, can contribute to hypoxic neuronal injury and blood-brain barrier dysfunction, respectively. Current therapeutics target pathological mechanisms by employing antivirals, decreasing inflammation, and promoting olfactory epithelium regeneration. Thus, from laboratory evidence and clinical trials in the literature, we sought to synthesize the pathophysiological pathways underlying neurological symptoms of long COVID and potential therapeutics.
Keywords: COVID-19; SARS-CoV-2; brain fog; long COVID; neurological complication; neurological manifestations; outcome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
