

A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor
- PMID: 36899963
- PMCID: PMC10001379
- DOI: 10.3390/diagnostics13050819
A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor
Abstract
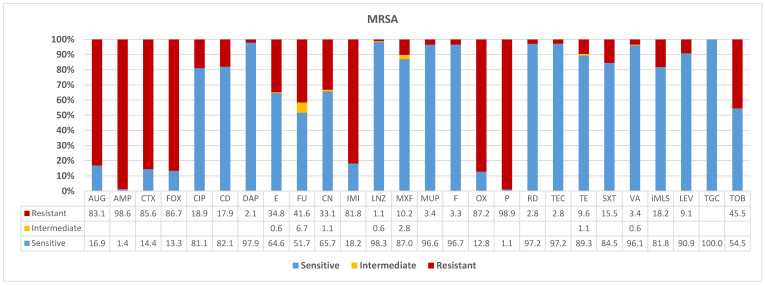
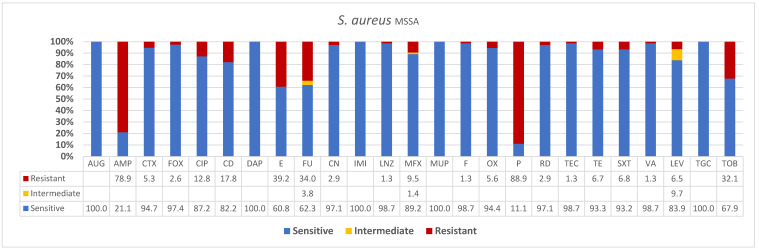
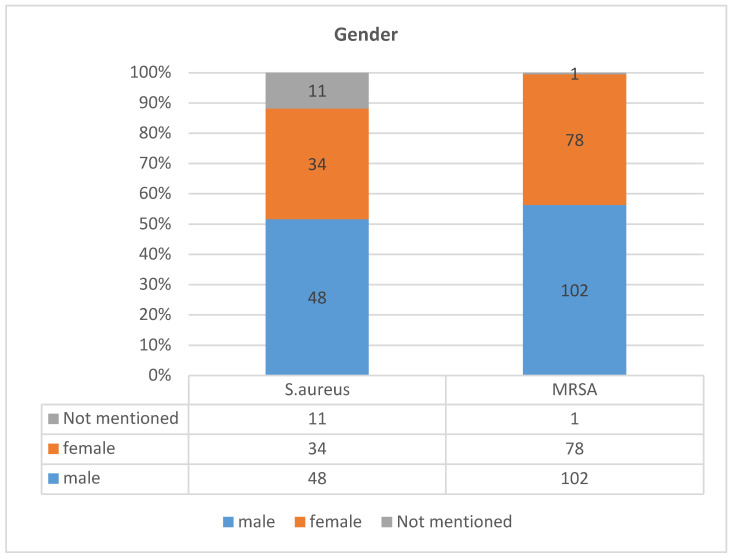
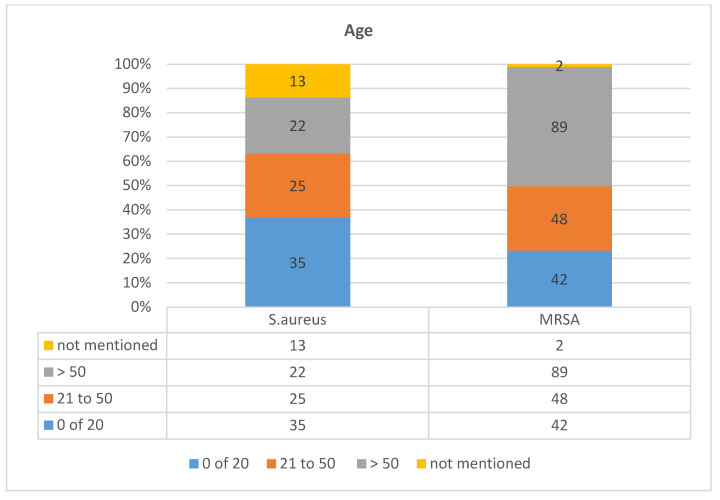
The rapidly changing epidemiology of Staphylococcus aureus and evolution of strains with enhanced virulence is a significant issue in global healthcare. Hospital-associated methicillin-resistant S. aureus (HA-MRSA) lineages are being completely replaced by community-associated S. aureus (CA-MRSA) in many regions. Surveillance programs tracing the reservoirs and sources of infections are needed. Using molecular diagnostics, antibiograms, and patient demographics, we have examined the distributions of S. aureus in Ha'il hospitals. Out of 274 S. aureus isolates recovered from clinical specimens, 181 (66%, n = 181) were MRSA, some with HA-MRSA patterns across 26 antimicrobials with almost full resistances to all beta-lactams, while the majority were highly susceptible to all non-beta-lactams, indicating the CA-MRSA type. The rest of isolates (34%, n = 93) were methicillin-susceptible, penicillin-resistant MSSA lineages (90%). The MRSA in men was over 56% among total MRSA (n = 181) isolates and 37% of overall isolates (n = 102 of 274) compared to MSSA in total isolates (17.5%, n = 48), respectively. However, these were 28.4% (n = 78) and 12.4% (n = 34) for MRSA and MSSA infections in women, respectively. MRSA rates per age groups of 0-20, 21-50, and >50 years of age were 15% (n = 42), 17% (n = 48), and 32% (n = 89), respectively. However, MSSA in the same age groups were 13% (n = 35), 9% (n = 25), and 8% (n = 22). Interestingly, MRSA increased proportional to age, while MSSA concomitantly decreased, implying dominance of the latter ancestors early in life and then gradual replacement by MRSA. The dominance and seriousness of MRSA despite enormous efforts in place is potentially for the increased use of beta-lactams known to enhance virulence. The Intriguing prevalence of the CA-MRSA patterns in young otherwise healthy individuals replaced by MRSA later in seniors and the dominance of penicillin-resistant MSSA phenotypes imply three types of host- and age-specific evolutionary lineages. Thus, the decreasing MSSA trend by age with concomitant increase and sub-clonal differentiation into HA-MRSA in seniors and CA-MRSA in young and otherwise healthy patients strongly support the notion of subclinal emergences from a resident penicillin-resistant MSSA ancestor. Future vertical studies should focus on the surveillance of invasive CA-MRSA rates and phenotypes.
Keywords: CA-MRSA; HA-MRSA; S. aureus epidemiology; nosocomial S. aureus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
MRSA Profiles Reveal Age- and Gender-Specificity in a Tertiary Care Hospital: High Burden in ICU Elderly and Emerging Community Patterns in Youth.Microorganisms. 2025 May 6;13(5):1078. doi: 10.3390/microorganisms13051078. Microorganisms. 2025. PMID: 40431251 Free PMC article.
-
Molecular and Source-Specific Profiling of Hospital Staphylococcus aureus Reveal Dominance of Skin Infection and Age-Specific Selections in Pediatrics and Geriatrics.Microorganisms. 2023 Jan 6;11(1):149. doi: 10.3390/microorganisms11010149. Microorganisms. 2023. PMID: 36677441 Free PMC article.
-
Antibiotic susceptibility and genomic variations in Staphylococcus aureus associated with Skin and Soft Tissue Infection (SSTI) disease groups.BMC Infect Dis. 2016 Jun 10;16:276. doi: 10.1186/s12879-016-1630-z. BMC Infect Dis. 2016. PMID: 27287530 Free PMC article.
-
[Infectivity-resistotype-genotype clustering of methicillin-resistant Staphylococcus aureus strains in the Central Blacksea Region of Turkey].Mikrobiyol Bul. 2014 Jan;48(1):14-27. Mikrobiyol Bul. 2014. PMID: 24506712 Turkish.
-
Bridges from hospitals to the laboratory: genetic portraits of methicillin-resistant Staphylococcus aureus clones.FEMS Immunol Med Microbiol. 2004 Mar 8;40(2):101-11. doi: 10.1016/S0928-8244(03)00370-5. FEMS Immunol Med Microbiol. 2004. PMID: 15040388 Review.
Cited by
-
MRSA Profiles Reveal Age- and Gender-Specificity in a Tertiary Care Hospital: High Burden in ICU Elderly and Emerging Community Patterns in Youth.Microorganisms. 2025 May 6;13(5):1078. doi: 10.3390/microorganisms13051078. Microorganisms. 2025. PMID: 40431251 Free PMC article.
-
MIC distribution analysis identifies differences in AMR between population sub-groups.Wellcome Open Res. 2024 May 9;9:244. doi: 10.12688/wellcomeopenres.21269.1. eCollection 2024. Wellcome Open Res. 2024. PMID: 39119595 Free PMC article.
-
An Overview of Antimicrobial Resistance in Saudi Arabia (2013-2023) and the Need for National Surveillance.Microorganisms. 2023 Aug 15;11(8):2086. doi: 10.3390/microorganisms11082086. Microorganisms. 2023. PMID: 37630646 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
