An official website of the United States government
The .gov means it’s official.
Federal government websites often end in .gov or .mil. Before
sharing sensitive information, make sure you’re on a federal
government site.
The site is secure.
The https:// ensures that you are connecting to the
official website and that any information you provide is encrypted
and transmitted securely.
Ascending aorta diseases represent an important cause of mortality worldwide. Notably, acute and chronic thoracic aorta pathologies have increased during the last years, but medical therapy does not seem to influence their natural history. Currently, although open surgery is the first choice of treatment, many patients are still rejected or have poor outcomes. In this scenario, endovascular treatment is raised as a valuable option. In this review we describe the limitations of conventional surgery and the state-of-art of endovascular ascending aorta repair.
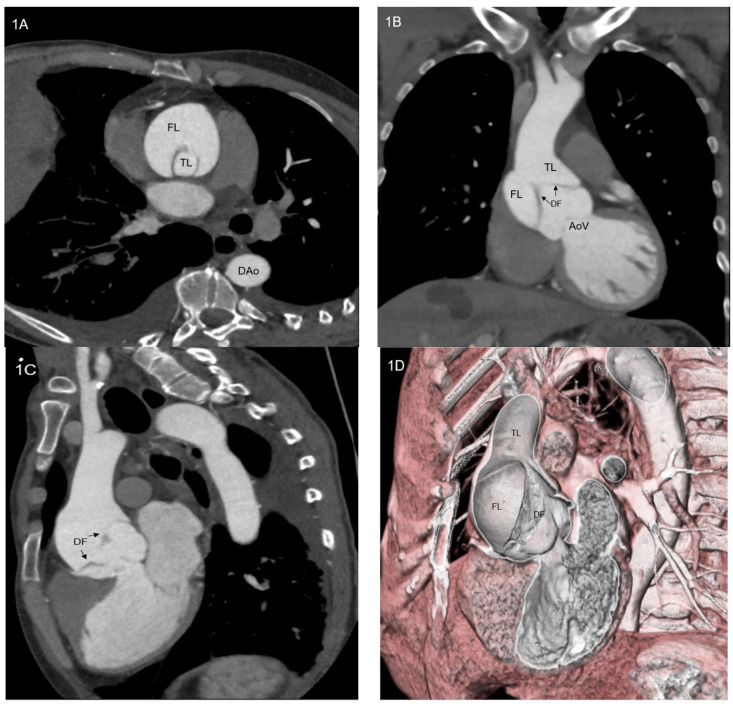
( A – D ) Computed tomography angiogram of a patient with type…
Figure 1
(A–D) Computed tomography angiogram of a patient with type A aortic dissection: axial scan (A), coronal scan (B), sagittal scan (C) and 3D volume rendering view. AoV = aortic valve; DAo = descending aorta; DF = dissection flap; FL = false lumen; TL = true lumen.
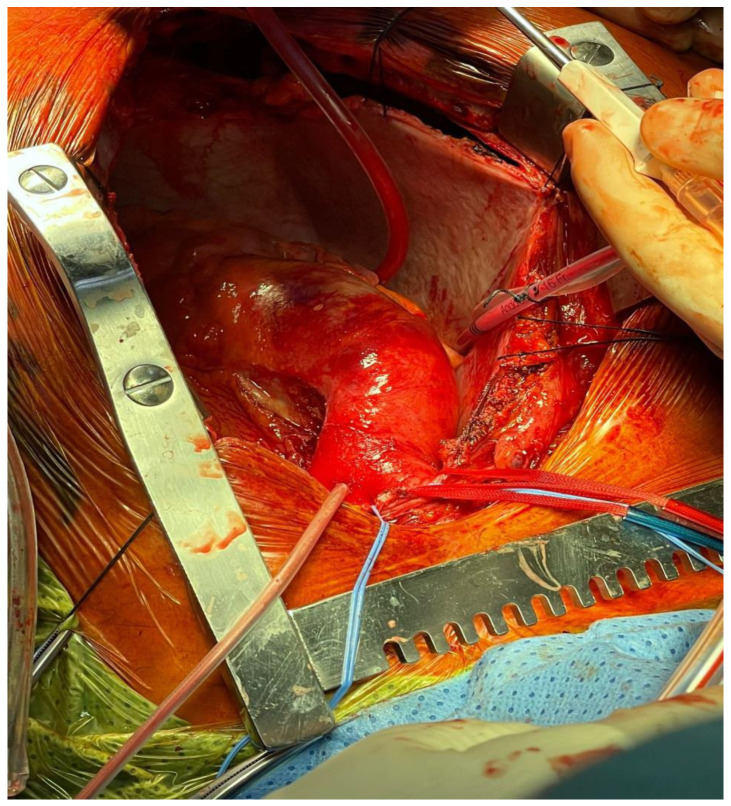
Figure 2
Real picture of type A…
Figure 2
Real picture of type A aortic dissection surgical repair after sternotomy.
Figure 2
Real picture of type A aortic dissection surgical repair after sternotomy.
Figure 3
Representation of type A aortic…
Figure 3
Representation of type A aortic dissection treated with a too long endoprosthesis, covering…
Figure 3
Representation of type A aortic dissection treated with a too long endoprosthesis, covering supra-aortic vessel origins. Red circle indicates supra-aortic vessel covering by the endoprosthesis. BCT = brachiocephalic trunk; FL = false lumen; LCCA = left common carotid artery; LMCA = left main coronary artery; LSA = left subclavian artery; RCA = right coronary artery.
Figure 4
Representation of type A aortic…
Figure 4
Representation of type A aortic dissection treated with a too short endoprosthesis that…
Figure 4
Representation of type A aortic dissection treated with a too short endoprosthesis that does not cover aortic dissection. Blue circle indicate the areas of dissection uncovered by endoprosthesis. BCT = brachiocephalic trunk; FL = false lumen; LCCA = left common carotid artery; LMCA = left main coronary artery; LSA = left subclavian artery; RCA = right coronary artery.
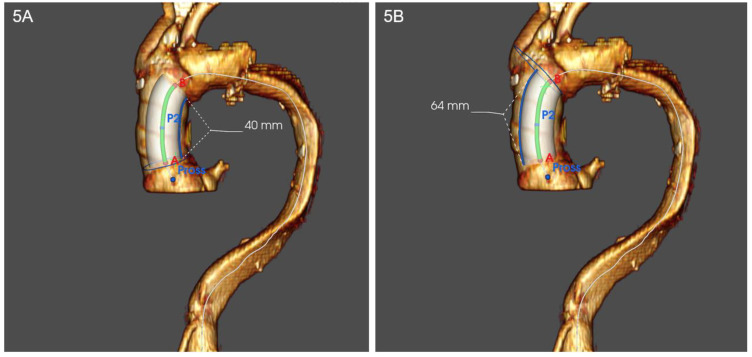
Figure 5
( A , B )…
Figure 5
( A , B ) Representation of inner and outer curves of ascending…
Figure 5
(A,B) Representation of inner and outer curves of ascending aorta in volume rendering 3D computed tomography angiogram. Inner curve (A) appears shorter than outer curve (B).
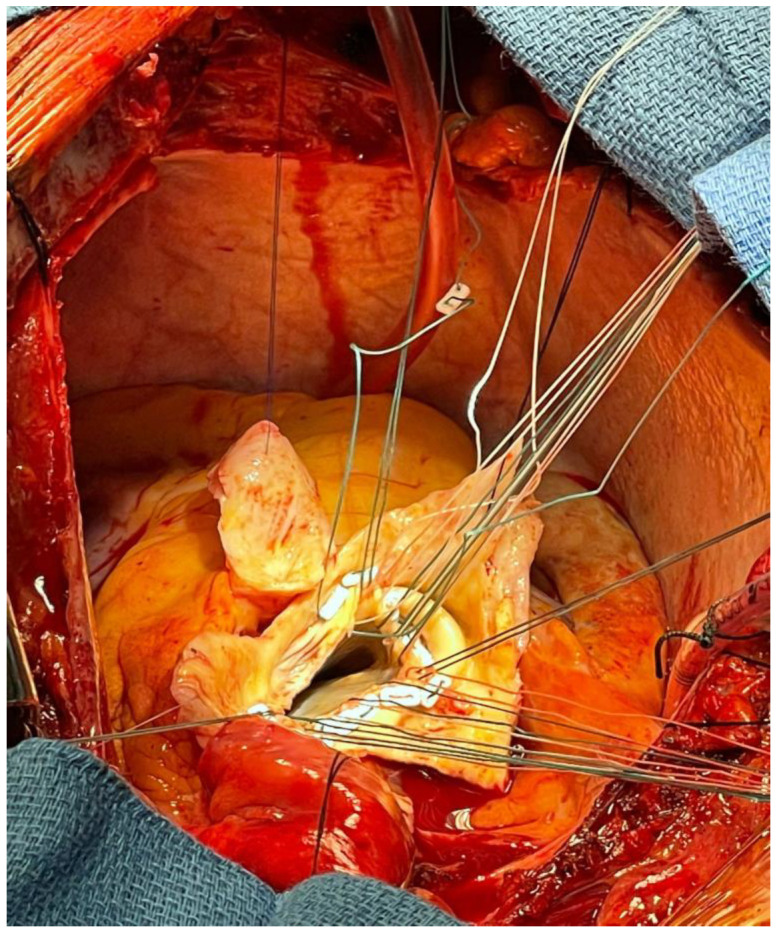
Figure 6
Real picture of Bentall intervention…
Figure 6
Real picture of Bentall intervention for type A aortic dissection complicated by aortic…
Figure 6
Real picture of Bentall intervention for type A aortic dissection complicated by aortic valve regurgitation, showing ascending aorta resection and aortic valve exposure.
Figure 7
Figure reporting the step-by-step procedure…
Figure 7
Figure reporting the step-by-step procedure published by Gaia in 2020. First, a femoral…
Figure 7
Figure reporting the step-by-step procedure published by Gaia in 2020. First, a femoral arterial access for angiography and femoral venous access for pacing are obtained; RCA and LMCA are cannulated; then a transapical access with a 30 Fr introducer is obtained; consequently, endoprosthesis is positioned and deployed; after that, balloon expandable prosthetic aortic valve is deployed. Then, RCA and LMCA are cannulated through endoprosthesis main body and coronary branches and connecting stents are finally deployed. Courtesy of Professor Diego Gaia, Federal University of Saõ Paulo, Brazil. LMCA = left main coronary artery; RCA = right coronary artery.
Heather B.P., Poskitt K.R., Earnshaw J.J., Whyman M., Shaw E. Population screening reduces mortality rate from aortic aneurysm in men. Br. J. Surg. 2000;87:750–753. doi: 10.1046/j.1365-2168.2000.01476.x.
-
DOI
-
PubMed
Scott R.A.P., Wilson N.M., A Ashton H., Kay D.N. Influence of screening on the incidence of ruptured abdominal aortic aneurysm: 5-year results of a randomized controlled study. Br. J. Surg. 1995;82:1066–1070. doi: 10.1002/bjs.1800820821.
-
DOI
-
PubMed
Olsson C., Thelin S., Ståhle E., Ekbom A., Granath F. Thoracic Aortic Aneurysm and Dissection. Circulation. 2006;114:2611–2618. doi: 10.1161/CIRCULATIONAHA.106.630400.
-
DOI
-
PubMed
Howard D.P., Banerjee A., Fairhead J.F., Perkins J., Silver L.E., Rothwell P.M. Population-Based Study of Incidence and Outcome of Acute Aortic Dissection and Premorbid Risk Factor Control. Circulation. 2013;127:2031–2037. doi: 10.1161/CIRCULATIONAHA.112.000483.
-
DOI
-
PMC
-
PubMed
Cheung C., Bernardo A.S., Trotter M.W.B., A Pedersen R., Sinha S. Generation of human vascular smooth muscle subtypes provides insight into embryological origin–dependent disease susceptibility. Nat. Biotechnol. 2012;30:165–173. doi: 10.1038/nbt.2107.
-
DOI
-
PMC
-
PubMed