

3.6 mW Active-Electrode ECG/ETI Sensor System Using Wideband Low-Noise Instrumentation Amplifier and High Impedance Balanced Current Driver
- PMID: 36904738
- PMCID: PMC10007594
- DOI: 10.3390/s23052536
3.6 mW Active-Electrode ECG/ETI Sensor System Using Wideband Low-Noise Instrumentation Amplifier and High Impedance Balanced Current Driver
Abstract
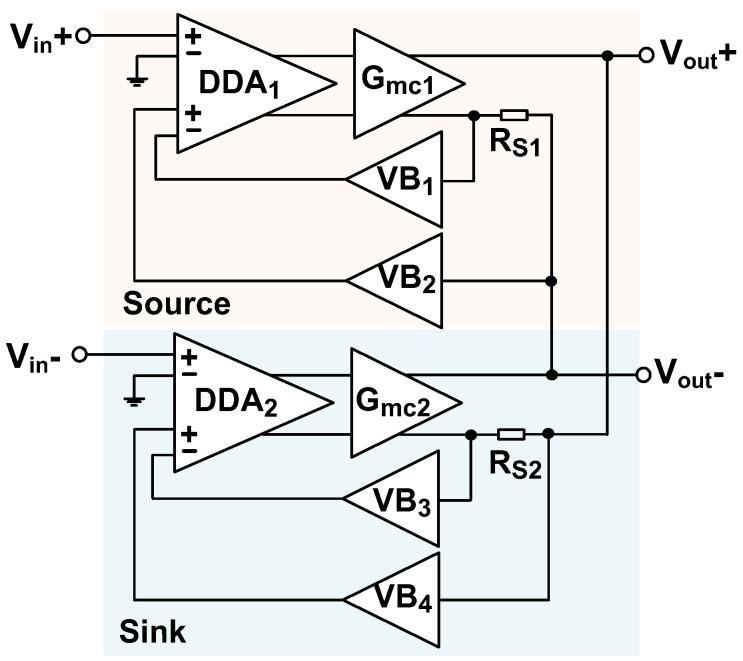
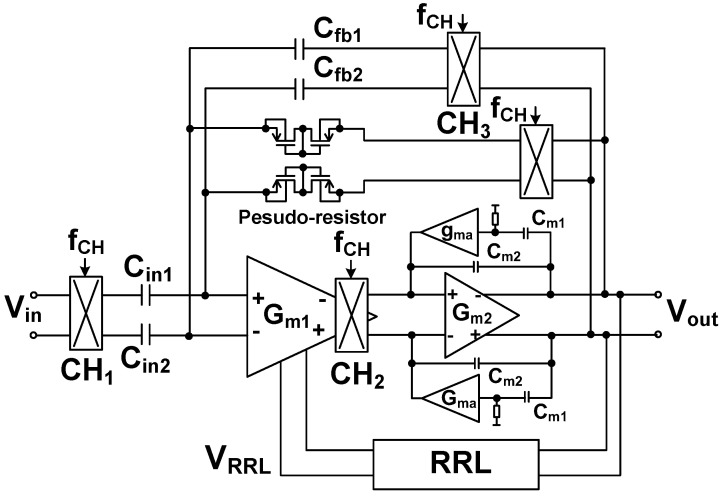
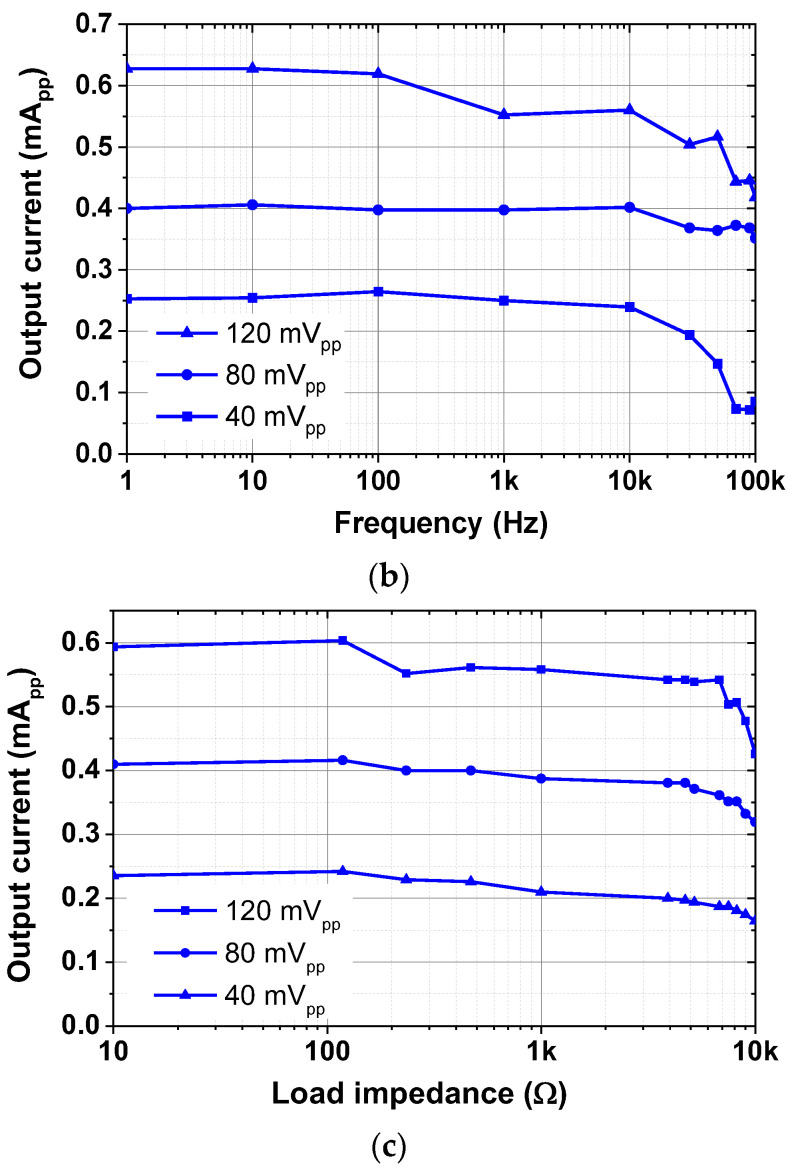
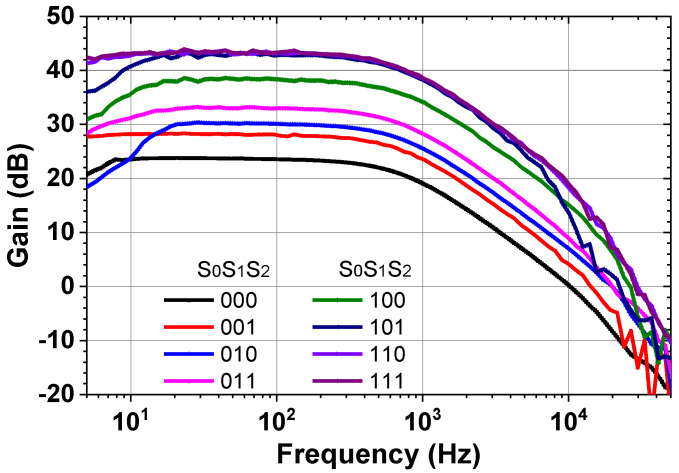
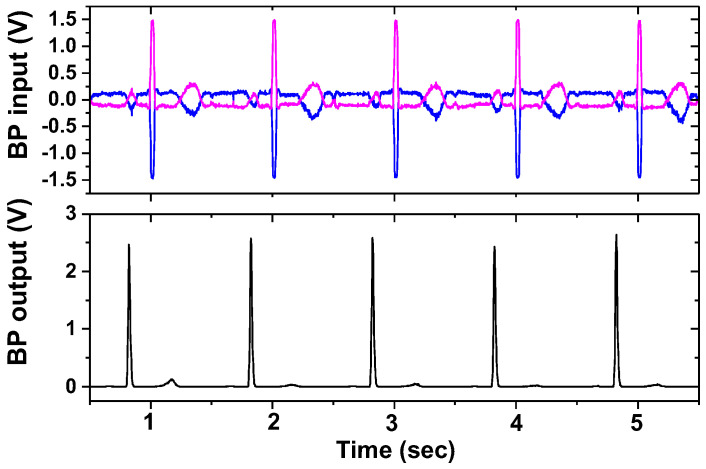
An active electrode (AE) and back-end (BE) integrated system for enhanced electrocardiogram (ECG)/electrode-tissue impedance (ETI) measurement is proposed. The AE consists of a balanced current driver and a preamplifier. To increase the output impedance, the current driver uses a matched current source and sink, which operates under negative feedback. To increase the linear input range, a new source degeneration method is proposed. The preamplifier is realized using a capacitively-coupled instrumentation amplifier (CCIA) with a ripple-reduction loop (RRL). Compared to the traditional Miller compensation, active frequency feedback compensation (AFFC) achieves bandwidth extension using the reduced size of the compensation capacitor. The BE performs three types of signal sensing: ECG, band power (BP), and impedance (IMP) data. The BP channel is used to detect the Q-, R-, and S-wave (QRS) complex in the ECG signal. The IMP channel measures the resistance and reactance of the electrode-tissue. The integrated circuits for the ECG/ETI system are realized in the 180 nm CMOS process and occupy a 1.26 mm2 area. The measured results show that the current driver supplies a relatively high current (>600 μApp) and achieves a high output impedance (1 MΩ at 500 kHz). The ETI system can detect resistance and capacitance in the ranges of 10 mΩ-3 kΩ and 100 nF-100 μF, respectively. The ECG/ETI system consumes 3.6 mW using a single 1.8 V supply.
Keywords: active electrode; bioimpedance; electrocardiogram; integrated circuit; preamplifier.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






















References
-
- Matthews R., Turner P.J., McDonald N.J., Ermolaev K., Mc Manus T., Shelby R.A., Steindorf M. Real time workload classification from an ambulatory wireless EEG system using hybrid EEG electrodes; Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society; Vancouver, BC, Canada. 20–25 August 2008; pp. 5871–5875. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
