

In silico modeling of patient-specific blood rheology in type 2 diabetes mellitus
- PMID: 36905122
- PMCID: PMC10147843
- DOI: 10.1016/j.bpj.2023.03.010
In silico modeling of patient-specific blood rheology in type 2 diabetes mellitus
Abstract
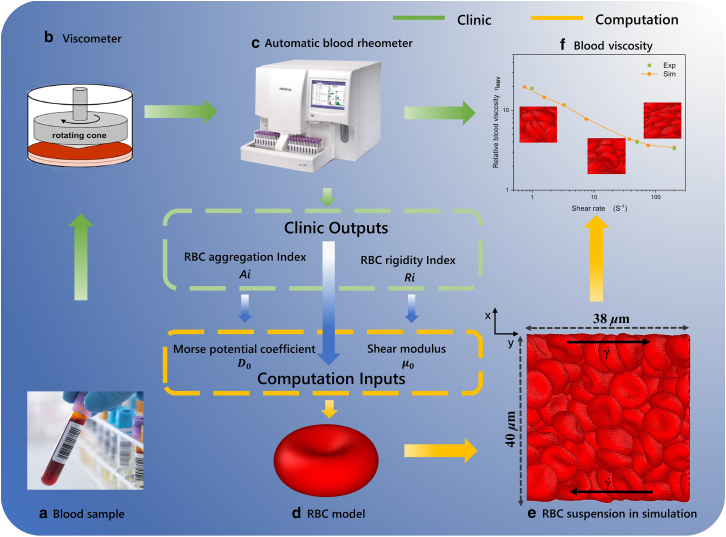
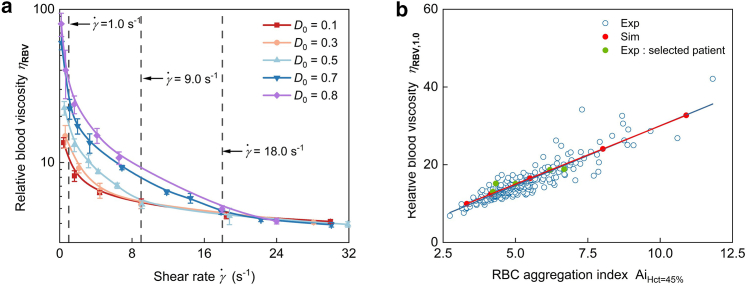
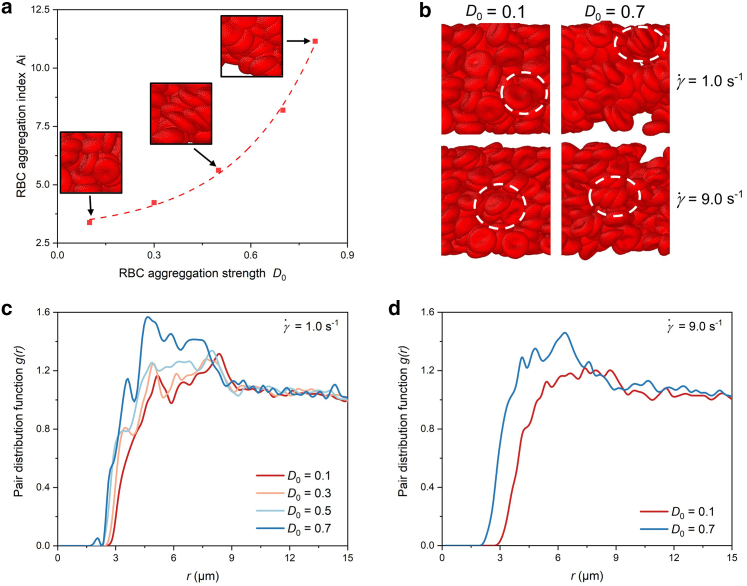
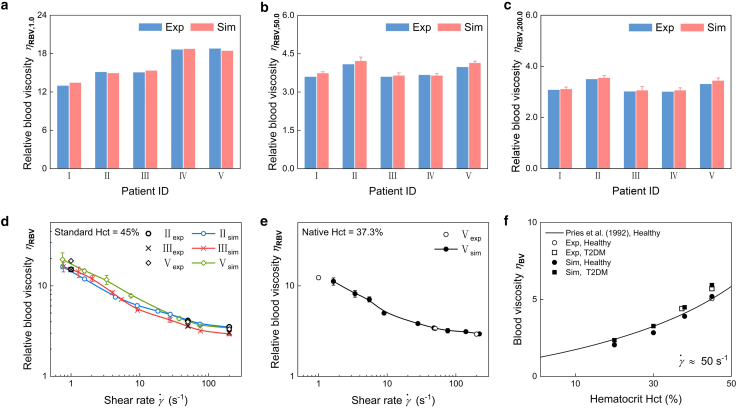
Increased blood viscosity in type 2 diabetes mellitus (T2DM) is a risk factor for the development of insulin resistance and diabetes-related vascular complications; however, individuals with T2DM exhibit heterogeneous hemorheological properties, including cell deformation and aggregation. Using a multiscale red blood cell (RBC) model with key parameters derived from patient-specific data, we present a computational study of the rheological properties of blood from individual patients with T2DM. Specifically, one key model parameter, which determines the shear stiffness of the RBC membrane (μ) is informed by the high-shear-rate blood viscosity of patients with T2DM. At the same time, the other, which contributes to the strength of the RBC aggregation interaction (D0), is derived from the low-shear-rate blood viscosity of patients with T2DM. The T2DM RBC suspensions are simulated at different shear rates, and the predicted blood viscosity is compared with clinical laboratory-measured data. The results show that the blood viscosity obtained from clinical laboratories and computational simulations are in agreement at both low and high shear rates. These quantitative simulation results demonstrate that the patient-specific model has truly learned the rheological behavior of T2DM blood by unifying the mechanical and aggregation factors of the RBCs, which provides an effective way to extract quantitative predictions of the rheological properties of the blood of individual patients with T2DM.
Copyright © 2023 Biophysical Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures



References
-
- Secomb T.W. Blood flow in the microcirculation. Annu. Rev. Fluid Mech. 2017;49:443–461.
-
- Baskurt O.K., Meiselman H.J. Blood rheology and hemodynamics. Semin. Thromb. Hemost. 2003;29:435–450. - PubMed
-
- Gnasso A., Cacia M., et al. Irace C. Influence of acute reduction of blood viscosity on endothelial function. Clin. Hemorheol. Microcirc. 2019;72:239–245. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
