

Characteristics of Immune Checkpoint Inhibitor-Associated Gastritis: Report from a Major Tertiary Care Center
- PMID: 36905577
- PMCID: PMC10400162
- DOI: 10.1093/oncolo/oyad031
Characteristics of Immune Checkpoint Inhibitor-Associated Gastritis: Report from a Major Tertiary Care Center
Abstract
Background: Immune checkpoint inhibitors (ICIs) have increased our ability to treat an ever-expanding number of cancers. We describe a case series of 25 patients who were diagnosed with gastritis following ICI therapy.
Materials and methods: This was a retrospective study involving 1712 patients treated for malignancy with immunotherapy at Cleveland Clinic from January 2011 to June 2019 (IRB 18-1225). We searched electronic medical records using ICD-10 codes for gastritis diagnosis confirmed on endoscopy and histology within 3 months of ICI therapy. Patients with upper gastrointestinal tract malignancy or documented Helicobacter pylori-associated gastritis were excluded.
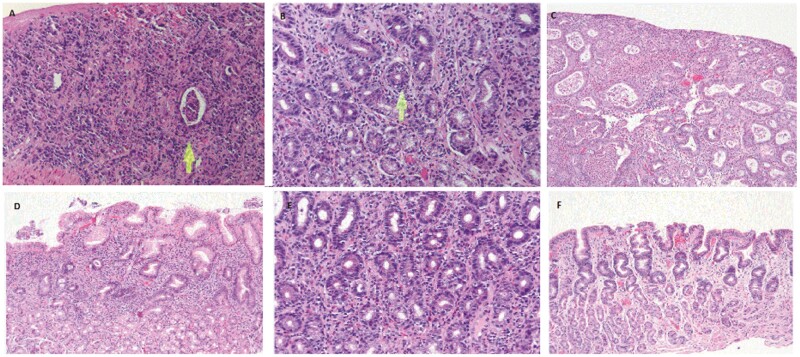
Results: Twenty-five patients were found to meet the criteria for diagnosis of gastritis. Of these 25 patients, most common malignancies were non-small cell lung cancer (52%) and melanoma (24%). Median number of infusions preceding symptoms was 4 (1-30) and time to symptom onset 2 (0.5-12) weeks after last infusion. Symptoms experienced were nausea (80%), vomiting (52%), abdominal pain (72%), and melena (44%). Common endoscopic findings were erythema (88%), edema (52%), and friability (48%). The most common diagnosis of pathology was chronic active gastritis in 24% of patients. Ninety-six percent received acid suppression treatment and 36% of patients also received steroids with an initial median dose of prednisone 75 (20-80) mg. Within 2 months, 64% had documented complete resolution of symptoms and 52% were able to resume immunotherapy.
Conclusion: Patients presenting with nausea, vomiting, abdominal pain, or melena following immunotherapy should be assessed for gastritis and if other causes are excluded, may require treatment as consideration for complication of immunotherapy.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
The authors indicated no financial relationships.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
