

Kidney Stone Prevention
- PMID: 36906146
- PMCID: PMC10201681
- DOI: 10.1016/j.advnut.2023.03.002
Kidney Stone Prevention
Abstract
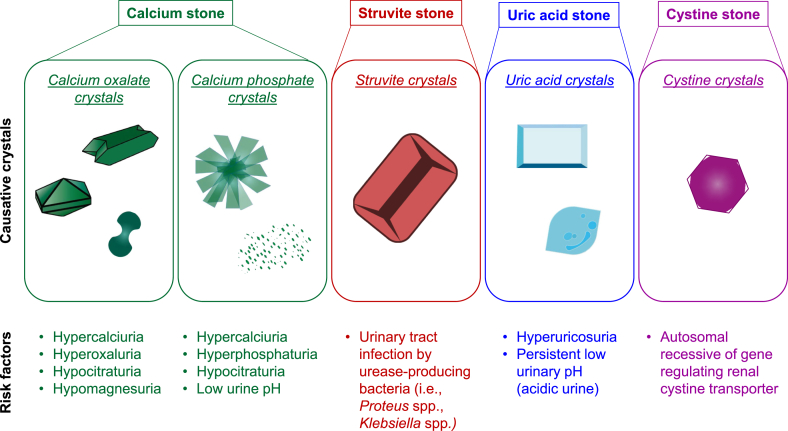
Kidney stone disease (KSD) (alternatively nephrolithiasis or urolithiasis) is a global health care problem that affects people in almost all of developed and developing countries. Its prevalence has been continuously increasing with a high recurrence rate after stone removal. Although effective therapeutic modalities are available, preventive strategies for both new and recurrent stones are required to reduce physical and financial burdens of KSD. To prevent kidney stone formation, its etiology and risk factors should be first considered. Low urine output and dehydration are the common risks of all stone types, whereas hypercalciuria, hyperoxaluria, and hypocitraturia are the major risks of calcium stones. In this article, up-to-date knowledge on strategies (nutrition-based mainly) to prevent KSD is provided. Important roles of fluid intake (2.5-3.0 L/d), diuresis (>2.0-2.5 L/d), lifestyle and habit modifications (for example, maintain normal body mass index, fluid compensation for working in high-temperature environment, and avoid cigarette smoking), and dietary management [for example, sufficient calcium at 1000-1200 mg/d, limit sodium at 2 or 3-5 g/d of sodium chloride (NaCl), limit oxalate-rich foods, avoid vitamin C and vitamin D supplements, limit animal proteins to 0.8-1.0 g/kg body weight/d but increase plant proteins in patients with calcium and uric acid stone and those with hyperuricosuria, increase proportion of citrus fruits, and consider lime powder supplementation] are summarized. Moreover, uses of natural bioactive products (for example, caffeine, epigallocatechin gallate, and diosmin), medications (for example, thiazides, alkaline citrate, other alkalinizing agents, and allopurinol), bacterial eradication, and probiotics are also discussed.
Keywords: bioactive compound; citrate; diuresis; natural compound; nephrolithiasis; probiotics; protection; urolithiasis.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
