

Immune Effector Cell-Associated Hemophagocytic Lymphohistiocytosis-Like Syndrome
- PMID: 36906275
- PMCID: PMC10330221
- DOI: 10.1016/j.jtct.2023.03.006
Immune Effector Cell-Associated Hemophagocytic Lymphohistiocytosis-Like Syndrome
Erratum in
-
Erratum to <Immune Effector Cell-Associated Hemophagocytic Lymphohistiocytosis-Like Syndrome><[Transplant Cell Ther. 2023 Jul;29(7):438.e1-438.e16. Epub 2023 Mar 9]>Transplant Cell Ther. 2025 Oct 30:S2666-6367(25)01440-X. doi: 10.1016/j.jtct.2025.09.016. Online ahead of print. Transplant Cell Ther. 2025. PMID: 41067707 Free PMC article. No abstract available.
Abstract
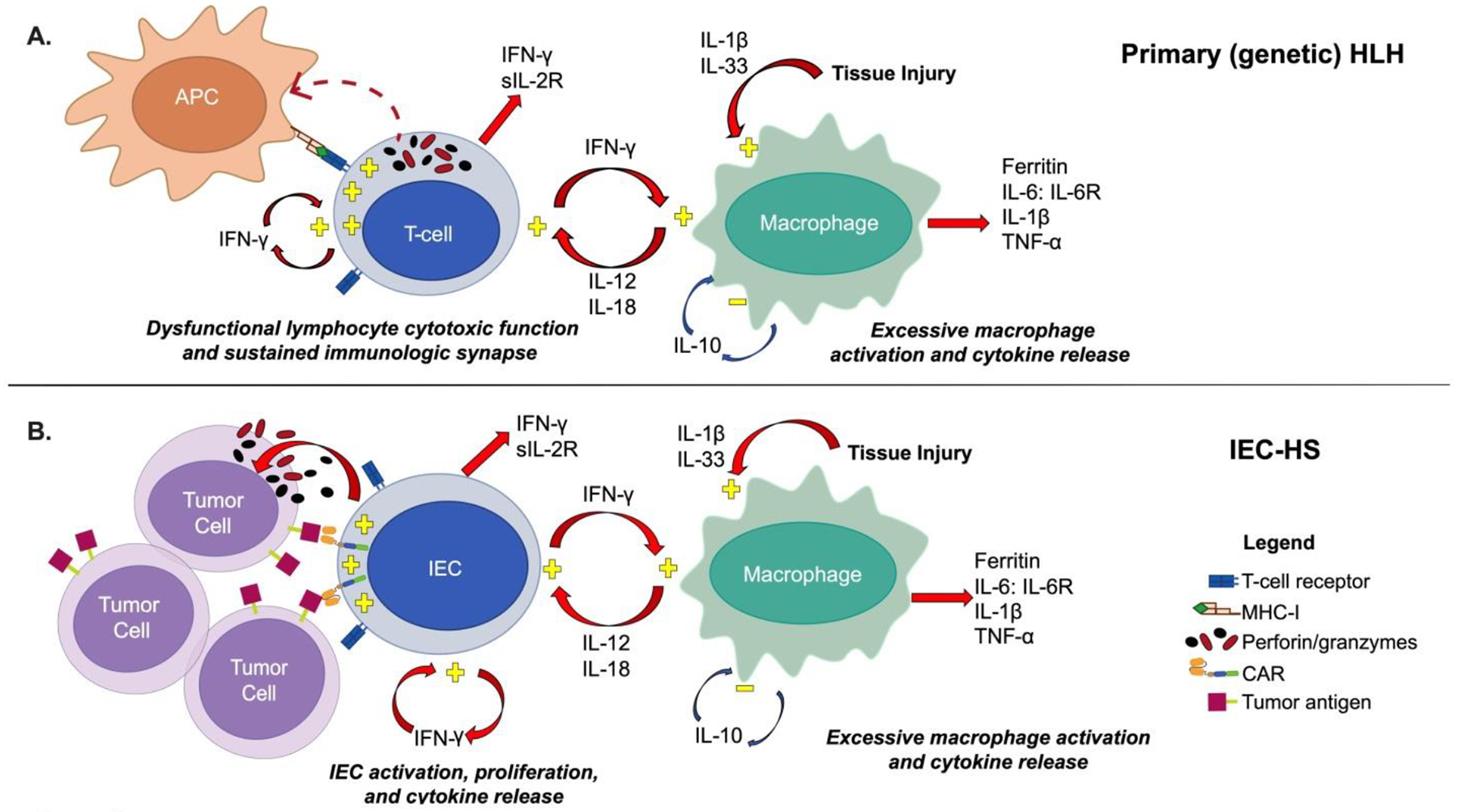
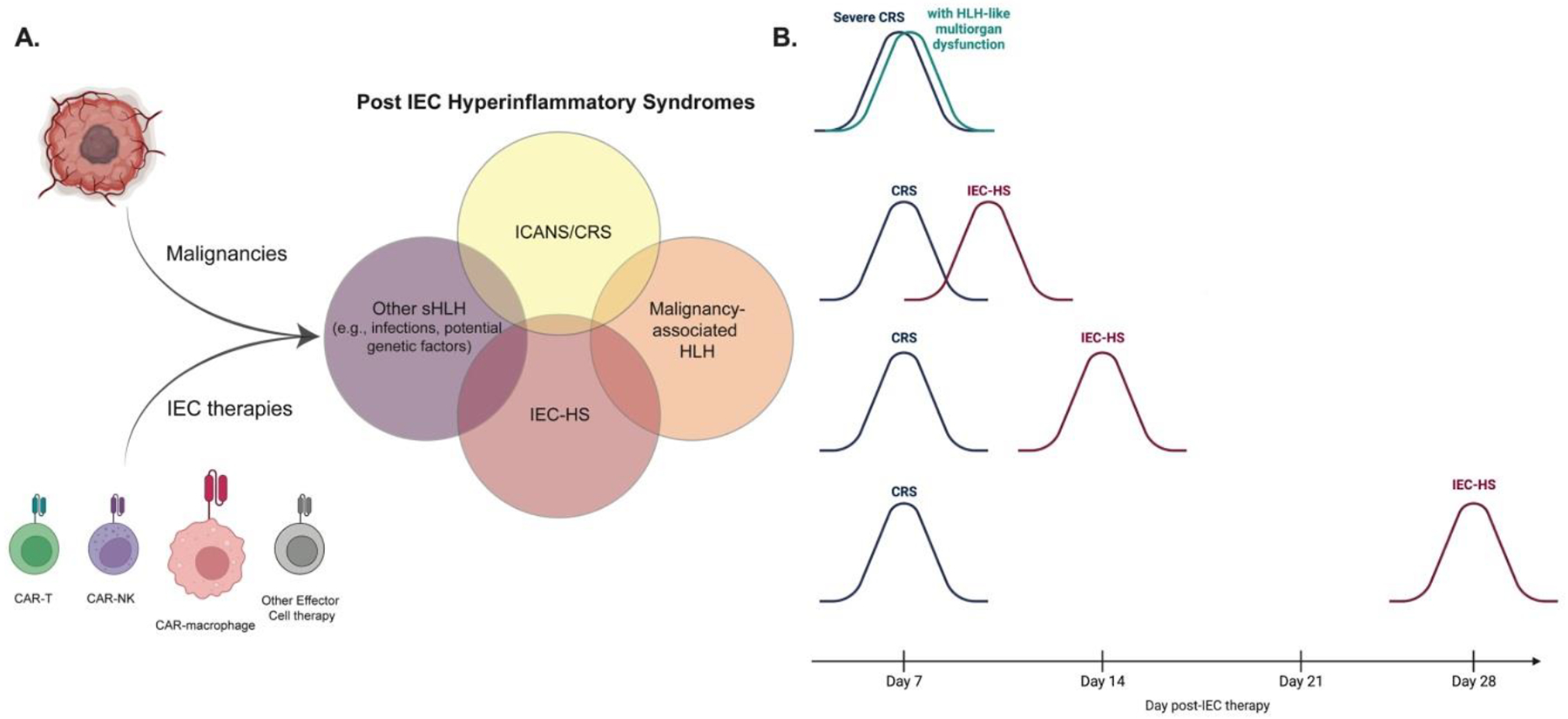
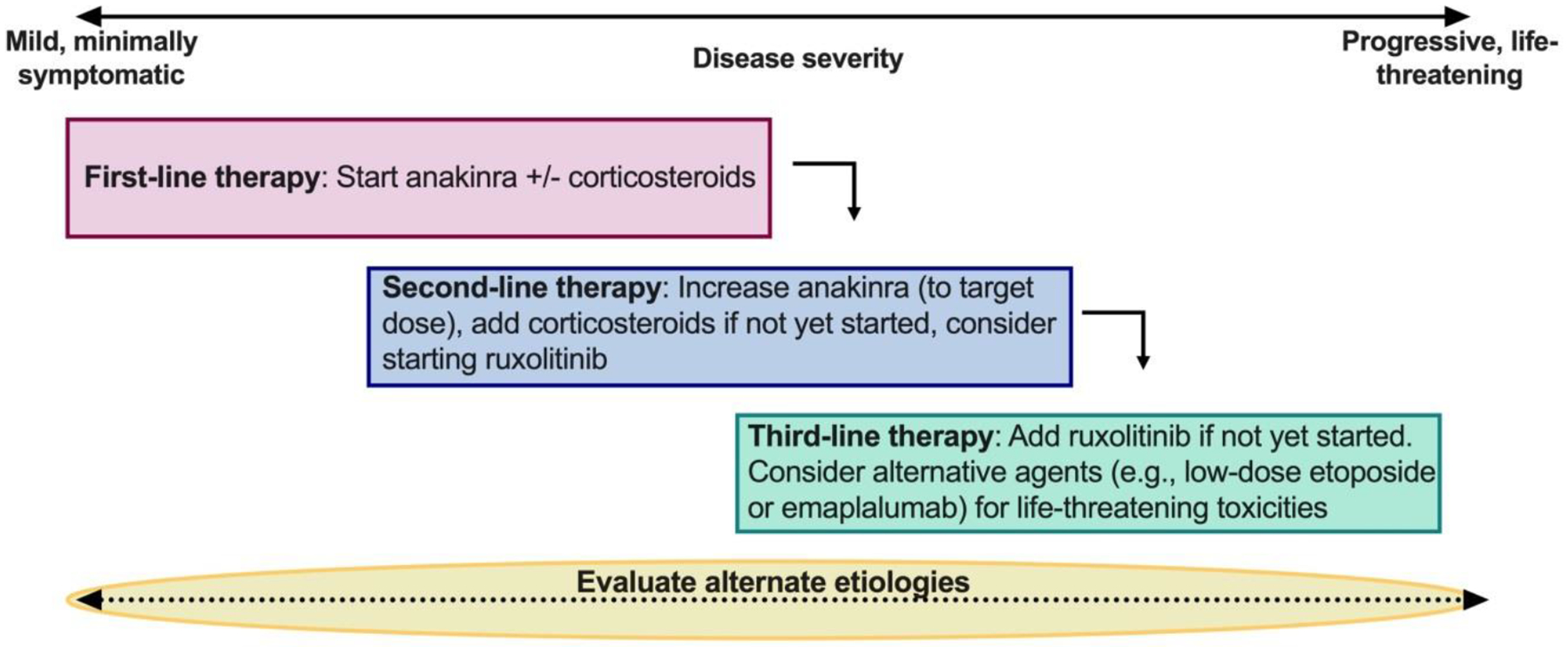
T cell-mediated hyperinflammatory responses, such as cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS), are now well-established toxicities of chimeric antigen receptor (CAR) T cell therapy. As the field of CAR T cells advances, however, there is increasing recognition that hemophagocytic lymphohistiocytosis (HLH)-like toxicities following CAR T cell infusion are occurring broadly across patient populations and CAR T cell constructs. Importantly, these HLH-like toxicities are often not as directly associated with CRS and/or its severity as initially described. This emergent toxicity, however ill-defined, is associated with life-threatening complications, creating an urgent need for improved identification and optimal management. With the goal of improving patient outcomes and formulating a framework to characterize and study this HLH-like syndrome, we established an American Society for Transplantation and Cellular Therapy panel composed of experts in primary and secondary HLH, pediatric and adult HLH, infectious disease, rheumatology and hematology, oncology, and cellular therapy. Through this effort, we provide an overview of the underlying biology of classical primary and secondary HLH, explore its relationship with similar manifestations following CAR T cell infusions, and propose the term "immune effector cell-associated HLH-like syndrome (IEC-HS)" to describe this emergent toxicity. We also delineate a framework for identifying IEC-HS and put forward a grading schema that can be used to assess severity and facilitate cross-trial comparisons. Additionally, given the critical need to optimize outcomes for patients experiencing IEC-HS, we provide insight into potential treatment approaches and strategies to optimize supportive care and delineate alternate etiologies that should be considered in a patient presenting with IEC-HS. By collectively defining IEC-HS as a hyperinflammatory toxicity, we can now embark on further study of the pathophysiology underlying this toxicity profile and make strides toward a more comprehensive assessment and treatment approach.
Keywords: Chimeric antigen receptor T cell; Hemophagocytic lymphohistiocytosis; Macrophage activation syndrome.
Published by Elsevier Inc.
Conflict of interest statement
The content of this publication does not necessarily reflect the views of policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government. This work was supported in part by the Intramural Research Program of the National Institutes of Health, National Cancer Institute, Center for Cancer Research and the Warren Grant Magnuson Clinical Center (ZIA BC 011823, N. Shah).
Dr. Nirali N Shah receives royalties from Cargo, Inc and has participated in Advisory Boards for Sobi and VOR.
Dr. Tania Jain receives institutional research support from CTI Biopharma, SyneosHealth, Incyte; Advisory board participation with Care Dx, Bristol Myers Squibb, Incyte, Abbvie, CTI, and Kite.
Dr. Perales reports honoraria from Adicet, Allovir, Caribou Biosciences, Celgene, Bristol-Myers Squibb, Equilium, Exevir, Incyte, Karyopharm, Kite/Gilead, Merck, Miltenyi Biotec, MorphoSys, Nektar Therapeutics, Novartis, Omeros, OrcaBio, Syncopation, VectivBio AG, and Vor Biopharma. He serves on DSMBs for Cidara Therapeutics, Medigene, and Sellas Life Sciences, and the scientific advisory board of NexImmune. He has ownership interests in NexImmune and Omeros. He has received institutional research support for clinical trials from Incyte, Kite/Gilead, Miltenyi Biotec, Nektar Therapeutics, and Novartis.
Dr Henter serves as a consultant for Sobi.
Dr. Michael Jain reports honoraria from Kite/Gilead, BMS, Novartis, and Myeloid Therapeutics. He reports research funding from Kite/Gilead and Incyte.
Dr. JA Hill reports honoraria from Gilead Sciences, Pfizer/Amplyx, Allovir, Allogene therapeutics, CRISPR therapeutics, CSL Behring, OptumHealth, Octapharma, Karius, and Takeda and research funding from Takeda, Allovir, Karius, Merck, Deverra, and Gilead Sciences, all unrelated to this manuscript. He reports no other relevant COI
Dr. Maron reports research funding from Astellas Inc and Symbio Pharma Inc, both unrelated to this manuscript
Dr. Hines receives institutional funding from Incyte for a clinical trial utilizing ruxolitinib for HLH.
Dr. Neelapu received research support from Kite/Gilead, BMS, Cellectis, Poseida, Allogene, Unum Therapeutics, Precision Biosciences, and Adicet Bio; served as Advisory Board Member/Consultant for Kite/Gilead, Merck, Novartis, Sellas Life Sciences, Athenex, Allogene, Incyte, Adicet Bio, BMS, Legend Biotech, Bluebird Bio, Fosun Kite, Sana Biotechnology, Caribou, Astellas Pharma, Morphosys, Janssen, Chimagen, ImmunoACT, and Orna Therapeutics; has received royalty income from Takeda Pharmaceuticals; has stock options from Longbow Immunotherapy, Inc; and has intellectual property related to cell therapy.
Dr. Nirav Shah reports participation on advisory boards and/or consultancy for Kite Pharma, BMS, TG therapeutics, Miltenyi Biotec, Lilly Oncology, Epizyme, Incyte, Novartis, Seattle Genetics, and Umoja. He has research funding and honoraria from Lilly Oncology and Miltenyi Biotec. In addition, N.S. is on a scientific advisory board for Tundra Therapeutics. These relationships are all unrelated to this manuscript
Dr Sairah Ahmed has research support to institution for clinical trials from Seattle Genetics, Merck, Xencor, Chimagen and Tessa Therapeutics, has membership on Tessa Therapeutic’s and Chimagen scientific advisory committee, she serves on Data Safety Monitoring Board for Myeloid Therapeutics; she is a consultant for ADC therapeutics, KITE/Gilead
Dr. Matthew Frigault reports consulting/honoraria from Kite/Gilead, Novartis, BMS, JnJ/Legend, Incyte, and Arcellx.
Dr. Mahadeo has served as a consultant and has received research support from Atara Biotherapuetics and Jazz.
Dr. Komanduri has served as an ad hoc consultant for Kite/Gilead, BMS, Novartis, Adaptimmune, Autolus, Janssen, Genentech, Cargo Therapeutics, Takeda, CRISPR, Incyte, Optum Health and the Bill and Melinda Gates Foundation. He serves on scientific advisory boards for Avacta Therapeutics and Aegle Therapeutics and as a voluntary member of the Board of Directors of the National Marrow Donor Program.
Dr. Frank has participated in Advisory Boards for Kite/Gilead and Cargo Inc and received research support from Adaptive Biotechnology and Allogene Biotechnologies
Dr. Nikiforow reports participation in ad hoc advisory boards for A2 Bio, GlaxoSmithKline, Iovance, Kite/Gilead and Sobi.
Figures
References
-
- La Rosee P, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465–2477. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
