

Adverse neonatal outcome and veno-arterial differences in umbilical cord blood pH (ΔpH) at birth: a population-based study of 108,629 newborns
- PMID: 36906543
- PMCID: PMC10007827
- DOI: 10.1186/s12884-023-05487-8
Adverse neonatal outcome and veno-arterial differences in umbilical cord blood pH (ΔpH) at birth: a population-based study of 108,629 newborns
Abstract
Background: Umbilical cord blood gases are routinely used by midwives and obstetricians for quality assurance of birth management and in clinical research. They can form the basis for solving medicolegal issues in the identification of severe intrapartum hypoxia at birth. However, the scientific value of veno-arterial differences in cord blood pH, also known as ΔpH, is largely unknown. By tradition, the Apgar score is frequently used to predict perinatal morbidity and mortality, however significant inter-observer and regional variations decrease its reliability and there is a need to identify more accurate markers of perinatal asphyxia. The aim of our study was to investigate the association of small and large veno-arterial differences in umbilical cord pH, ΔpH, with adverse neonatal outcome.
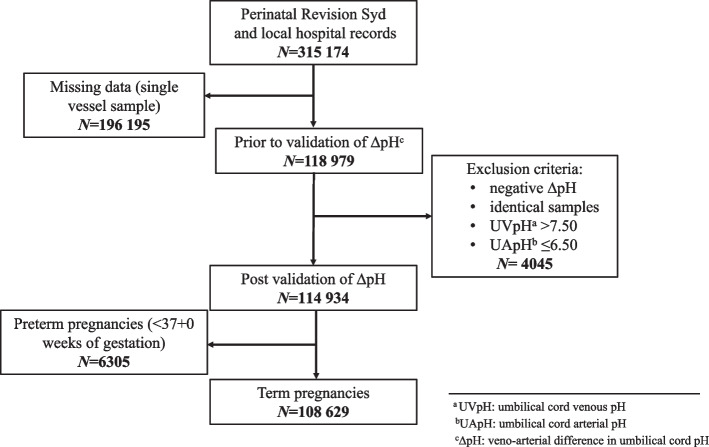
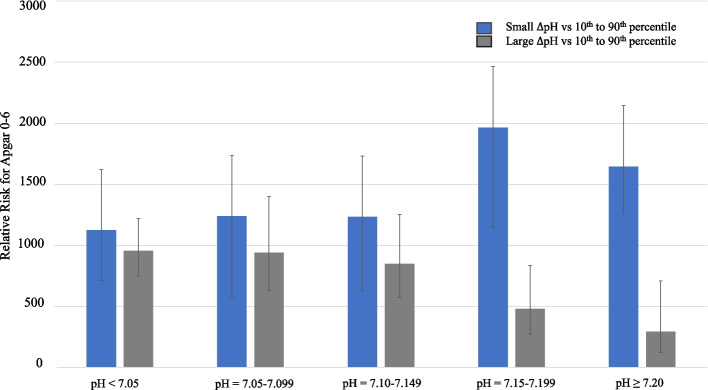
Methods: This retrospective, population-based study collected obstetric and neonatal data from women giving birth in nine maternity units from Southern Sweden from 1995 to 2015. Data was extracted from the Perinatal South Revision Register, a quality regional health database. Newborns at ≥37 gestational weeks with a complete and validated set of umbilical cord blood samples from both cord artery and vein were included. Outcome measures included: ΔpH percentiles, 'Small ΔpH' (10th percentile), 'Large ΔpH' (90th percentile), Apgar score (0-6), need for continuous positive airway pressure (CPAP) and admission to neonatal intensive care unit (NICU). Relative risks (RR) were calculated with modified Poisson regression model.
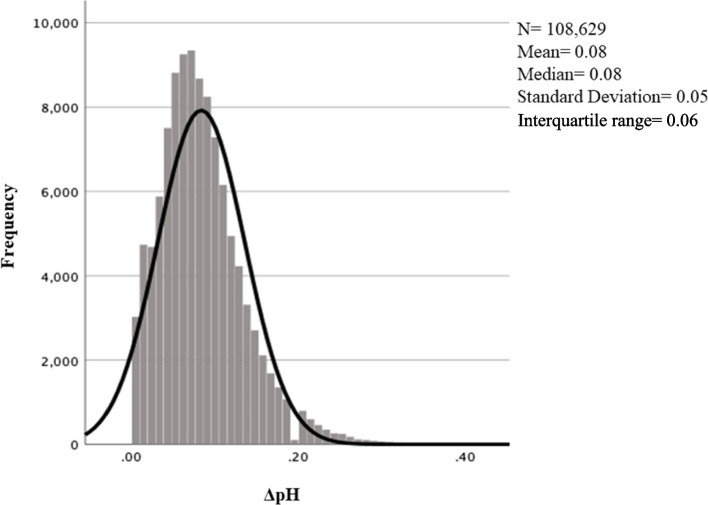
Results: The study population comprised of 108,629 newborns with complete and validated data. Mean and median ΔpH was 0.08 ± 0.05. Analyses of RR showed that 'Large ΔpH' was associated with a decreased RR of adverse perinatal outcome with increasing UApH (at UApH ≥7.20: RR for low Apgar 0.29, P = 0.01; CPAP 0.55, P = 0.02; NICU admission 0.81, P = 0.01). 'Small ΔpH' was associated with an increased RR for low Apgar score and NICU admission only at higher UApH values (at UApH 7.15-7.199: RR for low Apgar 1.96, P = 0.01; at UApH ≥7.20: RR for low Apgar 1.65, P = 0.00, RR for NICU admission 1.13, P = 0.01).
Conclusion: Large differences between cord venous and arterial pH (ΔpH) at birth were associated with a lower risk for perinatal morbidity including low 5-minute Apgar Score, the need for continuous positive airway pressure and NICU admission when UApH was above 7.15. Clinically, ΔpH may be a useful tool in the assessment of the newborn's metabolic condition at birth. Our findings may stem from the ability of the placenta to adequately replenish acid-base balance in fetal blood. 'Large ΔpH' may therefore be a marker of effective gas exchange in the placenta during birth.
Keywords: Adverse neonatal outcome; Apgar score; Birth; Birth asphyxia; Continuous positive airway pressure; Neonatal intensive care unit; Neonatal morbidity; Perinatal asphyxia; Umbilical artery pH; Umbilical cord blood gases; Umbilical cord pH.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Umbilical cord pH, blood gases, and lactate at birth: normal values, interpretation, and clinical utility.Am J Obstet Gynecol. 2023 May;228(5S):S1222-S1240. doi: 10.1016/j.ajog.2022.07.001. Epub 2023 Mar 19. Am J Obstet Gynecol. 2023. PMID: 37164495 Review.
-
Routine assessment of cerebroplacental ratio at 35-37 weeks' gestation in the prediction of adverse perinatal outcome.Am J Obstet Gynecol. 2019 Jul;221(1):65.e1-65.e18. doi: 10.1016/j.ajog.2019.03.002. Epub 2019 Mar 13. Am J Obstet Gynecol. 2019. PMID: 30878322
-
Umbilical cord pH and base excess values in relation to adverse outcome events for infants delivering at term.Am J Obstet Gynecol. 2004 Dec;191(6):2021-8. doi: 10.1016/j.ajog.2004.04.026. Am J Obstet Gynecol. 2004. PMID: 15592286
-
Acidemia in neonates with a 5-minute Apgar score of 7 or greater - What are the outcomes?Am J Obstet Gynecol. 2016 Oct;215(4):486.e1-6. doi: 10.1016/j.ajog.2016.05.035. Epub 2016 May 31. Am J Obstet Gynecol. 2016. PMID: 27255470
-
[Amniotic fluid insulin levels versus mean maternal blood glucose levels in gestational diabetes mellitus: an analysis of the neonatal outcome].Gynakol Geburtshilfliche Rundsch. 2009;49(4):249-53. doi: 10.1159/000301081. Epub 2010 May 19. Gynakol Geburtshilfliche Rundsch. 2009. PMID: 20530937 Review. German.
Cited by
-
Improving UK data on avoidable perinatal brain injury: review of data dictionaries and consultation.Pediatr Res. 2025 Jan 30. doi: 10.1038/s41390-025-03842-3. Online ahead of print. Pediatr Res. 2025. PMID: 39885238
References
-
- ACOG Committee opinion no. 348, November 2006: umbilical cord blood gas and acid-base analysis. Obstet Gynecol. 2006;108(5):1319–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
