

Effects of gastroesophageal reflux disease treatment with proton pump inhibitors on the risk of acute exacerbation and pneumonia in patients with COPD
- PMID: 36906585
- PMCID: PMC10008570
- DOI: 10.1186/s12931-023-02345-1
Effects of gastroesophageal reflux disease treatment with proton pump inhibitors on the risk of acute exacerbation and pneumonia in patients with COPD
Abstract
Background: Gastroesophageal reflux disease (GERD) has been suggested as a risk factor for acute exacerbation of chronic obstructive pulmonary disease (COPD). However, it remains undetermined whether proton pump inhibitor (PPI) treatment reduces the risk of exacerbation or affects the risk of pneumonia. This study aimed to evaluate the risks of both exacerbation and pneumonia following PPI treatment for GERD in patients with COPD.
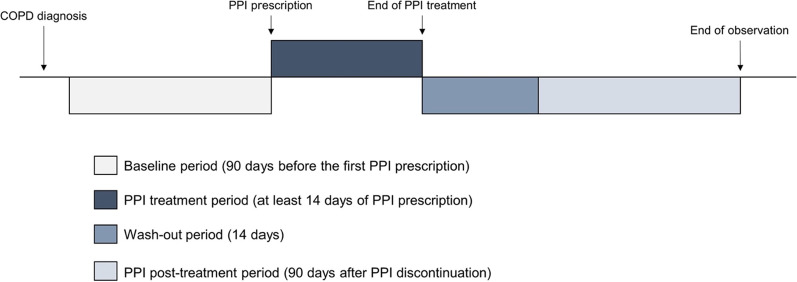
Methods: This study used a reimbursement database of the Republic of Korea. Patients aged ≥ 40 years with COPD as a main diagnosis and who received PPI treatment for GERD at least for 14 consecutive days between January 2013 and December 2018 were included in the study. A self-controlled case series analysis was conducted to calculate the risk of moderate and severe exacerbation and pneumonia.
Results: A total of 104,439 patients with prevalent COPD received PPI treatment for GERD. The risk of moderate exacerbation was significantly lower during the PPI treatment than at baseline. The risk of severe exacerbation increased during the PPI treatment but significantly decreased in the post-treatment period. Pneumonia risk was not significantly increased during the PPI treatment. The results were similar in patients with incident COPD.
Conclusions: The risk of exacerbation was significantly reduced after PPI treatment compared with the non-treated period. Severe exacerbation may increase due to uncontrolled GERD but subsequently decrease following PPI treatment. There was no evidence of an increased risk of pneumonia.
Keywords: Acute exacerbation; Chronic obstructive pulmonary disease; Gastroesophageal reflux disease; Pneumonia; Proton pump inhibitor.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Therapy with proton-pump inhibitors for gastroesophageal reflux disease does not reduce the risk for severe exacerbations in COPD.Respirology. 2016 Jul;21(5):883-90. doi: 10.1111/resp.12758. Epub 2016 Mar 11. Respirology. 2016. PMID: 26970108
-
Proton pump inhibitors use is associated with a lower risk of acute exacerbation and mortality in patients with coexistent COPD and GERD.Int J Chron Obstruct Pulmon Dis. 2018 Sep 19;13:2907-2915. doi: 10.2147/COPD.S157761. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30275689 Free PMC article.
-
Proton pump inhibitors for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2020 Aug 25;8(8):CD013113. doi: 10.1002/14651858.CD013113.pub2. Cochrane Database Syst Rev. 2020. PMID: 32844430 Free PMC article.
-
Associations between gastro-oesophageal reflux, its management and exacerbations of chronic obstructive pulmonary disease.Respir Med. 2015 Sep;109(9):1147-54. doi: 10.1016/j.rmed.2015.06.009. Epub 2015 Jun 23. Respir Med. 2015. PMID: 26166017
-
ARE THE PERSISTENT SYMPTOMS TO PROTON PUMP INHIBITOR THERAPY DUE TO REFRACTORY GASTROESOPHAGEAL REFLUX DISEASE OR TO OTHER DISORDERS?Arq Gastroenterol. 2018 Nov;55Suppl 1(Suppl 1):85-91. doi: 10.1590/S0004-2803.201800000-48. Epub 2018 Oct 4. Arq Gastroenterol. 2018. PMID: 30304291 Review.
Cited by
-
Treatable traits identified in Chinese patients hospitalized with AECOPD: A Multicenter Cohort Study.Int J Med Sci. 2025 Apr 13;22(9):2227-2236. doi: 10.7150/ijms.111294. eCollection 2025. Int J Med Sci. 2025. PMID: 40303489 Free PMC article.
-
Causal relationship between gastroesophageal reflux disease and chronic obstructive respiratory disease: A bidirectional Mendelian randomization study.Heliyon. 2025 Jan 18;11(2):e42100. doi: 10.1016/j.heliyon.2025.e42100. eCollection 2025 Jan 30. Heliyon. 2025. PMID: 39906855 Free PMC article.
-
Common gastrointestinal diseases and chronic obstructive pulmonary disease risk: a bidirectional Mendelian randomization analysis.Front Genet. 2023 Nov 16;14:1256833. doi: 10.3389/fgene.2023.1256833. eCollection 2023. Front Genet. 2023. PMID: 38046045 Free PMC article.
-
Subtypes of Patients with Mild to Moderate Airflow Limitation as Predictors of Chronic Obstructive Pulmonary Disease Exacerbation.J Clin Med. 2023 Oct 20;12(20):6643. doi: 10.3390/jcm12206643. J Clin Med. 2023. PMID: 37892781 Free PMC article.
-
Proton Pump Inhibitor Use and Its Association with Lung Cancer Likelihood and Mortality: A Nationwide Nested Case-Control Study in Korea.Cancers (Basel). 2025 Mar 4;17(5):877. doi: 10.3390/cancers17050877. Cancers (Basel). 2025. PMID: 40075724 Free PMC article.
References
-
- Global strategy for prevention, diagnosis and management of COPD. https://goldcopd.org/2021-gold-reports/.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
