

Limitation of life-sustaining therapies in critically ill patients with COVID-19: a descriptive epidemiological investigation from the COVID-ICU study
- PMID: 36906643
- PMCID: PMC10006561
- DOI: 10.1186/s13054-023-04349-1
Limitation of life-sustaining therapies in critically ill patients with COVID-19: a descriptive epidemiological investigation from the COVID-ICU study
Abstract
Background: Limitations of life-sustaining therapies (LST) practices are frequent and vary among intensive care units (ICUs). However, scarce data were available during the COVID-19 pandemic when ICUs were under intense pressure. We aimed to investigate the prevalence, cumulative incidence, timing, modalities, and factors associated with LST decisions in critically ill COVID-19 patients.
Methods: We did an ancillary analysis of the European multicentre COVID-ICU study, which collected data from 163 ICUs in France, Belgium and Switzerland. ICU load, a parameter reflecting stress on ICU capacities, was calculated at the patient level using daily ICU bed occupancy data from official country epidemiological reports. Mixed effects logistic regression was used to assess the association of variables with LST limitation decisions.
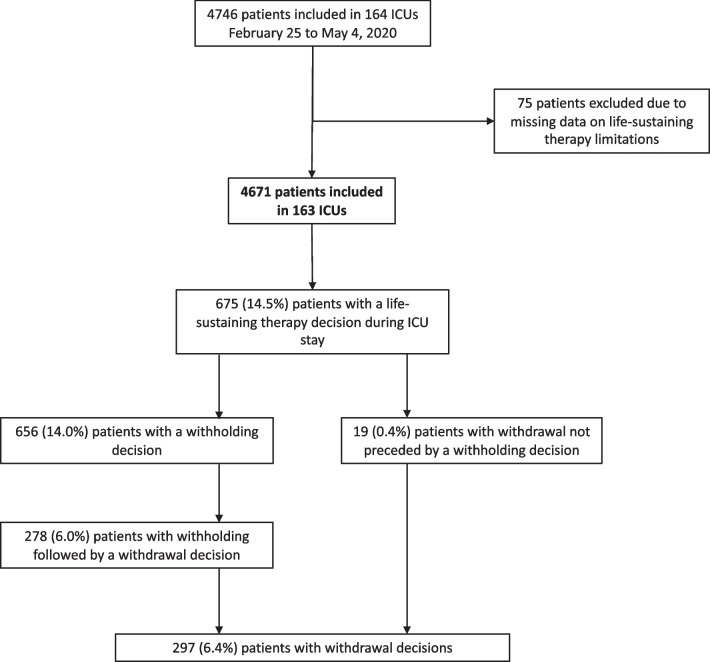
Results: Among 4671 severe COVID-19 patients admitted from February 25 to May 4, 2020, the prevalence of in-ICU LST limitations was 14.5%, with a nearly six-fold variability between centres. Overall 28-day cumulative incidence of LST limitations was 12.4%, which occurred at a median of 8 days (3-21). Median ICU load at the patient level was 126%. Age, clinical frailty scale score, and respiratory severity were associated with LST limitations, while ICU load was not. In-ICU death occurred in 74% and 95% of patients, respectively, after LST withholding and withdrawal, while median survival time was 3 days (1-11) after LST limitations.
Conclusions: In this study, LST limitations frequently preceded death, with a major impact on time of death. In contrast to ICU load, older age, frailty, and the severity of respiratory failure during the first 24 h were the main factors associated with decisions of LST limitations.
Keywords: Acute respiratory distress syndrome; COVID-19; Critical care; Ethical; Life-sustaining therapy; Outcome.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Comment in
-
Limitation of life‑sustaining therapies in critically ill patients with COVID‑19: What lessons to draw?Crit Care. 2023 May 22;27(1):195. doi: 10.1186/s13054-023-04470-1. Crit Care. 2023. PMID: 37218008 Free PMC article. No abstract available.
References
-
- Bravata DM, Perkins AJ, Myers LJ, Arling G, Zhang Y, Zillich AJ, et al. Association of intensive care unit patient load and demand with mortality rates in us department of veterans affairs hospitals during the COVID-19 pandemic. JAMA Netw Open. 2021;4:e2034266. doi: 10.1001/jamanetworkopen.2020.34266. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
