

Pediatric Myocarditis
- PMID: 36906691
- PMCID: PMC10008072
- DOI: 10.1007/s40119-023-00309-6
Pediatric Myocarditis
Abstract
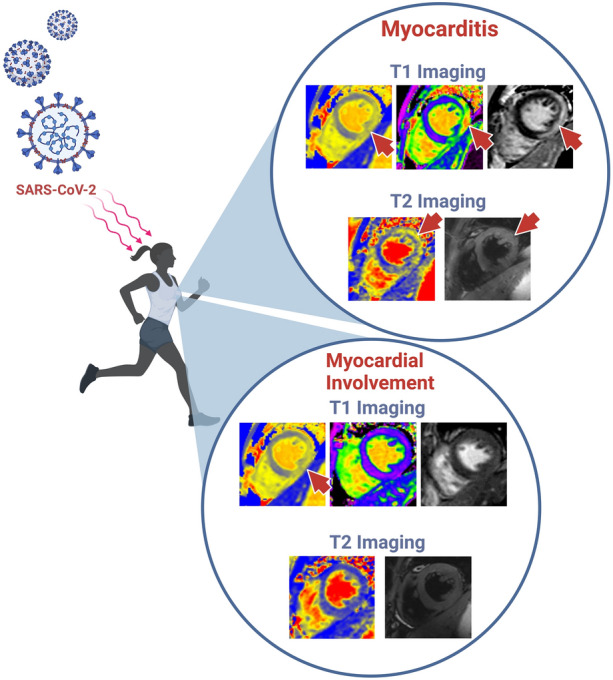
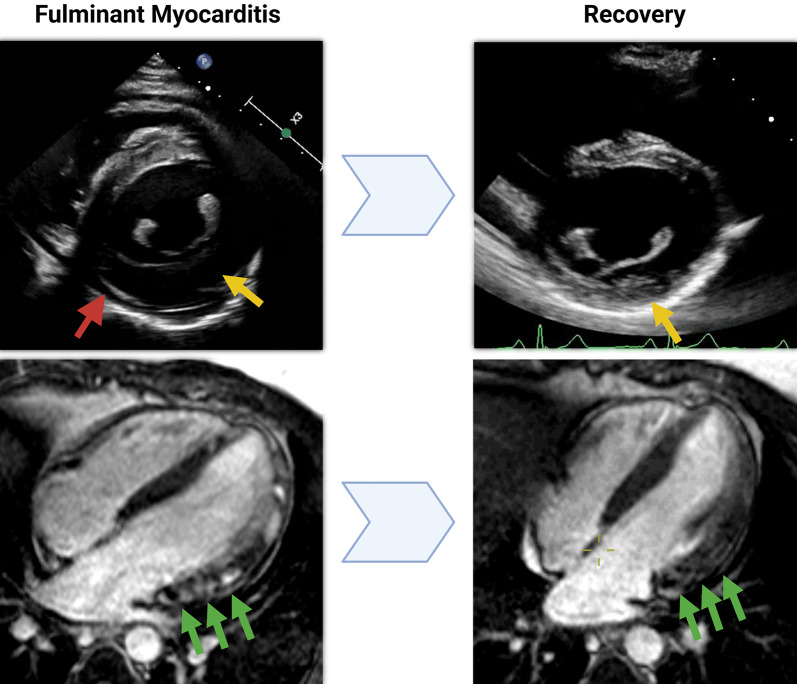
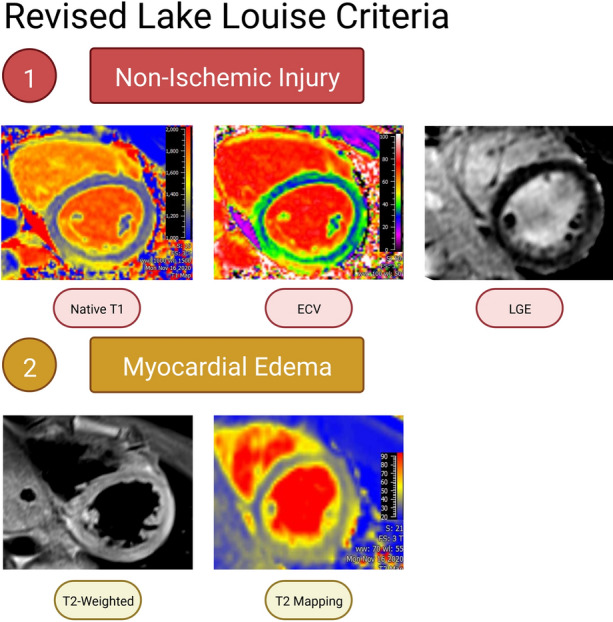
Myocarditis is a condition caused by acute or chronic inflammation of the cardiac myocytes, resulting in associated myocardial edema and myocardial injury or necrosis. The exact incidence is unknown, but is likely underestimated, with more mild cases going unreported. Diagnosis and appropriate management are paramount in pediatric myocarditis, as it remains a recognized cause of sudden cardiac death in children and athletes. Myocarditis in children is most often caused by a viral or infectious etiology. In addition, there are now two highly recognized etiologies related to Coronavirus disease of 2019 (COVID-19) infection and the COVID-19 mRNA vaccine. The clinic presentation of children with myocarditis can range from asymptomatic to critically ill. Related to severe acute respiratory syndrome-Coronavirus 2 (SARs-CoV-2), children are at greater risk of developing myocarditis secondary to COVID-19 compared to the mRNA COVID-19 vaccine. Diagnosis of myocarditis typically includes laboratory testing, electrocardiography (ECG), chest X-ray, and additional non-invasive imaging studies with echocardiogram typically being the first-line imaging modality. While the reference standard for diagnosing myocarditis was previously endomyocardial biopsy, with the new revised Lake Louise Criteria, cardiac magnetic resonance (CMR) has emerged as an integral non-invasive imaging tool to assist in the diagnosis. CMR remains critical, as it allows for assessment of ventricular function and tissue characterization, with newer techniques, such as myocardial strain, to help guide management both acutely and long term.
Keywords: CMR; COVID-19; Lake Louise Criteria; MIS-C; Myocarditis; Pediatric; SARs-CoV-2.
© 2023. The Author(s).
Conflict of interest statement
Jason L. Williams, Hannah M. Jacobs, and Simon Lee have nothing to disclose.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
