

Comparison of paediatric emergency department visits for attempted suicide, self-harm, and suicidal ideation before and during the COVID-19 pandemic: a systematic review and meta-analysis
- PMID: 36907199
- PMCID: PMC10097509
- DOI: 10.1016/S2215-0366(23)00036-6
Comparison of paediatric emergency department visits for attempted suicide, self-harm, and suicidal ideation before and during the COVID-19 pandemic: a systematic review and meta-analysis
Abstract
Background: There is a lack of consensus about the effect of the COVID-19 pandemic on the mental health of children and adolescents. We aimed to compare rates of paediatric emergency department visits for attempted suicide, self-harm, and suicidal ideation during the pandemic with those before the pandemic.
Methods: For this systematic review and meta-analysis, we searched MEDLINE, Embase, and PsycINFO for studies published between Jan 1, 2020, and Dec 19, 2022. Studies published in English with data on paediatric (ie, those aged <19 years) emergency department visits before and during the COVID-19 pandemic were included. Case studies and qualitative analyses were excluded. Changes in attempted suicide, self-harm, suicidal ideation, and other mental-illness indicators (eg, anxiety, depression, and psychosis) were expressed as ratios of the rates of emergency department visits during the pandemic compared with those before the pandemic, and we analysed these with a random-effects meta-analysis. This study was registered with PROSPERO, CRD42022341897.
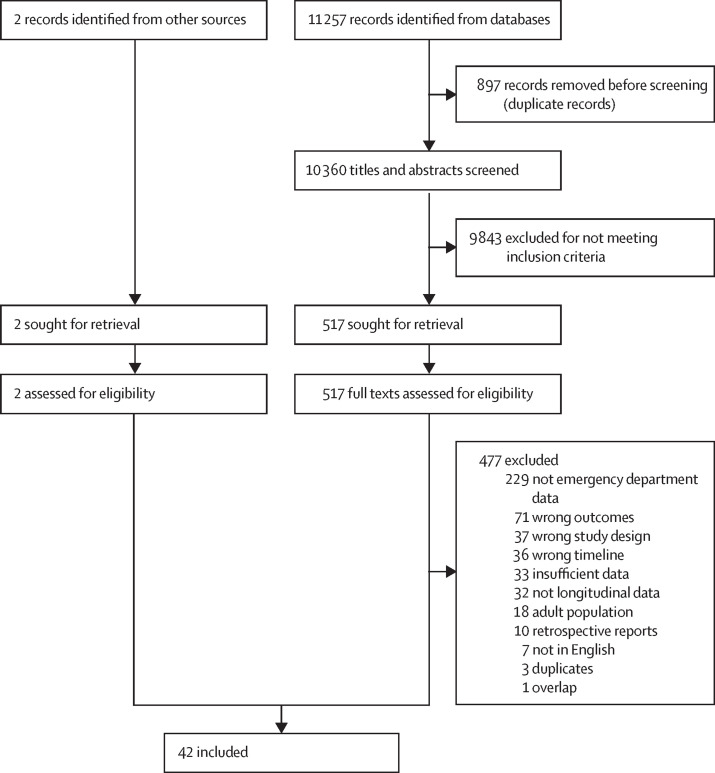
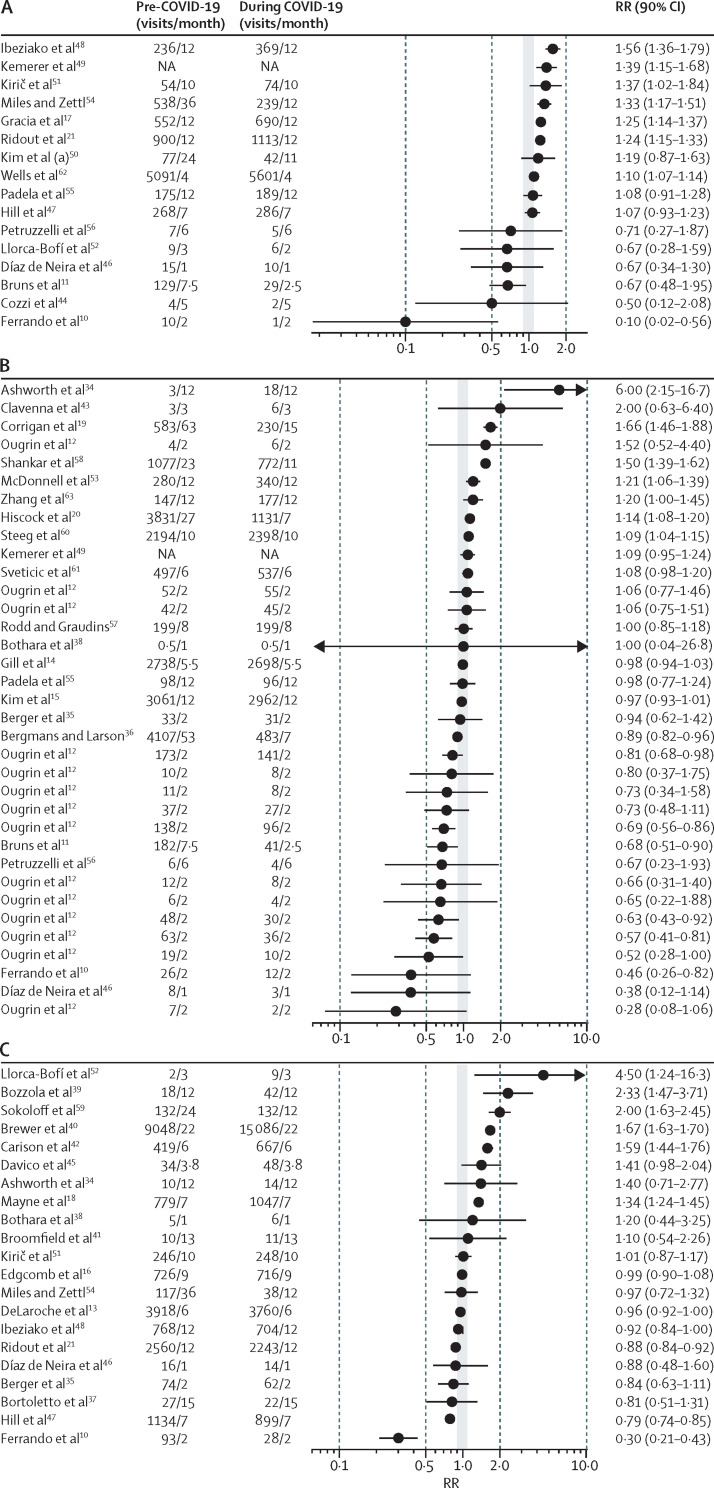
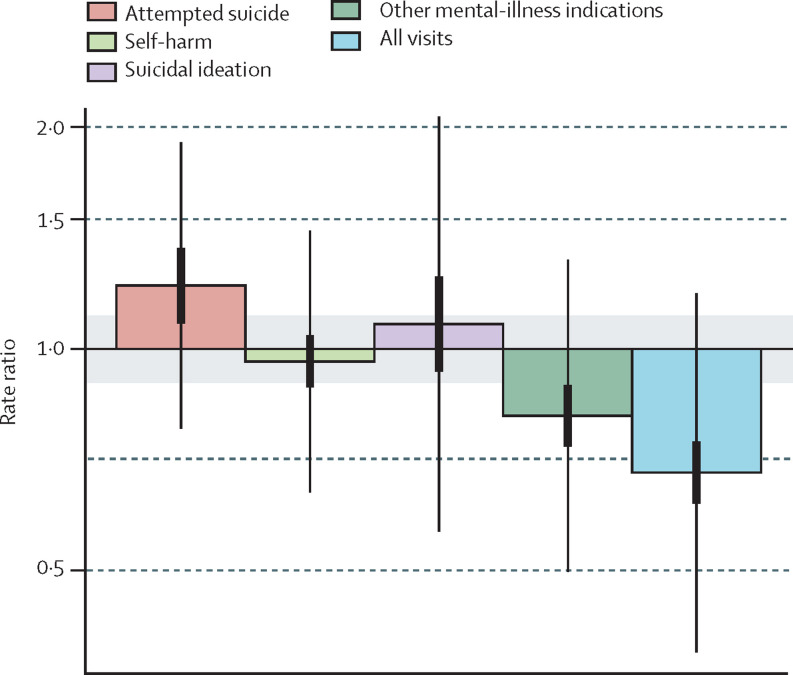
Findings: 10 360 non-duplicate records were retrieved, which yielded 42 relevant studies (with 130 sample-estimates) representing 11·1 million emergency department visits for all indications of children and adolescents across 18 countries. The mean age of the samples of children and adolescents across studies was 11·7 years (SD 3·1, range 5·5-16·3), and there were on average 57·6% girls and 43·4% boys as a proportion of emergency department visits for any health reasons (ie, physical and mental). Only one study had data related to race or ethnicity. There was good evidence of an increase in emergency department visits for attempted suicide during the pandemic (rate ratio 1·22, 90% CI 1·08-1·37), modest evidence of an increase in emergency department visits for suicidal ideation (1·08, 0·93-1·25), and good evidence for only a slight change in self-harm (0·96, 0·89-1·04). Rates of emergency department visits for other mental-illness indications showed very good evidence of a decline (0·81, 0·74-0·89), and paediatric visits for all health indications showed strong evidence of a reduction (0·68, 0·62-0·75). When rates for attempted suicide and suicidal ideation were combined as a single measure, there was good evidence of an increase in emergency department visits among girls (1·39, 1·04-1·88) and only modest evidence of an increase among boys (1·06, 0·92-1·24). Self-harm among older children (mean age 16·3 years, range 13·0-16·3) showed good evidence of an increase (1·18, 1·00-1·39), but among younger children (mean age 9·0 years, range 5·5-12·0) there was modest evidence of a decrease (0·85, 0·70-1·05).
Interpretation: The integration of mental health support within community health and the education system-including promotion, prevention, early intervention, and treatment-is urgently needed to increase the reach of mental health support that can mitigate child and adolescent mental distress. In future pandemics, increased resourcing in some emergency department settings would help to address their expected increase in visits for acute mental distress among children and adolescents.
Funding: None.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests TV has received honoraria for presentations related to youth suicide during the pandemic and is also the Chair of the COVID-19 Task Force and the Children and Schools working group for the Royal Society of Canada and is the President of the International Society for Research on Aggression. DJK has received grant funding related to research on youth suicide from the Canadian Institutes of Health Research, Sobey's Foundation, and SickKids Foundation in the past 36 months. All other authors declare no competing interests.
Figures
Comment in
-
Increasing paediatric emergency visits for suicide-related concerns during COVID-19.Lancet Psychiatry. 2023 May;10(5):308-309. doi: 10.1016/S2215-0366(23)00073-1. Epub 2023 Mar 9. Lancet Psychiatry. 2023. PMID: 36907198 Free PMC article. No abstract available.
-
COVID-19, young people, and suicidal behaviour.Lancet Psychiatry. 2023 Jul;10(7):483-484. doi: 10.1016/S2215-0366(23)00140-2. Lancet Psychiatry. 2023. PMID: 37353258 Free PMC article. No abstract available.
-
COVID-19, young people, and suicidal behaviour.Lancet Psychiatry. 2023 Jul;10(7):484-485. doi: 10.1016/S2215-0366(23)00159-1. Lancet Psychiatry. 2023. PMID: 37353259 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
