

Unravelling the potential of social prescribing in individual-level type 2 diabetes prevention: a mixed-methods realist evaluation
- PMID: 36907857
- PMCID: PMC10008720
- DOI: 10.1186/s12916-023-02796-9
Unravelling the potential of social prescribing in individual-level type 2 diabetes prevention: a mixed-methods realist evaluation
Abstract
Background: Social prescribing (SP) usually involves linking patients in primary care with services provided by the voluntary and community sector. Preliminary evidence suggests that SP may offer a means of connecting patients with community-based health promotion activities, potentially contributing to the prevention of long-term conditions, such as type 2 diabetes (T2D).
Methods: Using mixed-methods realist evaluation, we explored the possible contribution of SP to individual-level prevention of T2D in a multi-ethnic, socio-economically deprived population in London, UK. We made comparisons with an existing prevention programme (NHS Diabetes Prevention Programme (NDPP)) where relevant and possible. Anonymised primary care electronic health record data of 447,360 people 18+ with an active GP registration between December 2016 and February 2022 were analysed using quantitative methods. Qualitative data (interviews with 11 primary care clinicians, 11 social prescribers, 13 community organisations and 8 SP users at high risk of T2D; 36 hours of ethnographic observations of SP and NDPP sessions; and relevant documents) were analysed thematically. Data were integrated using visual means and realist methods.
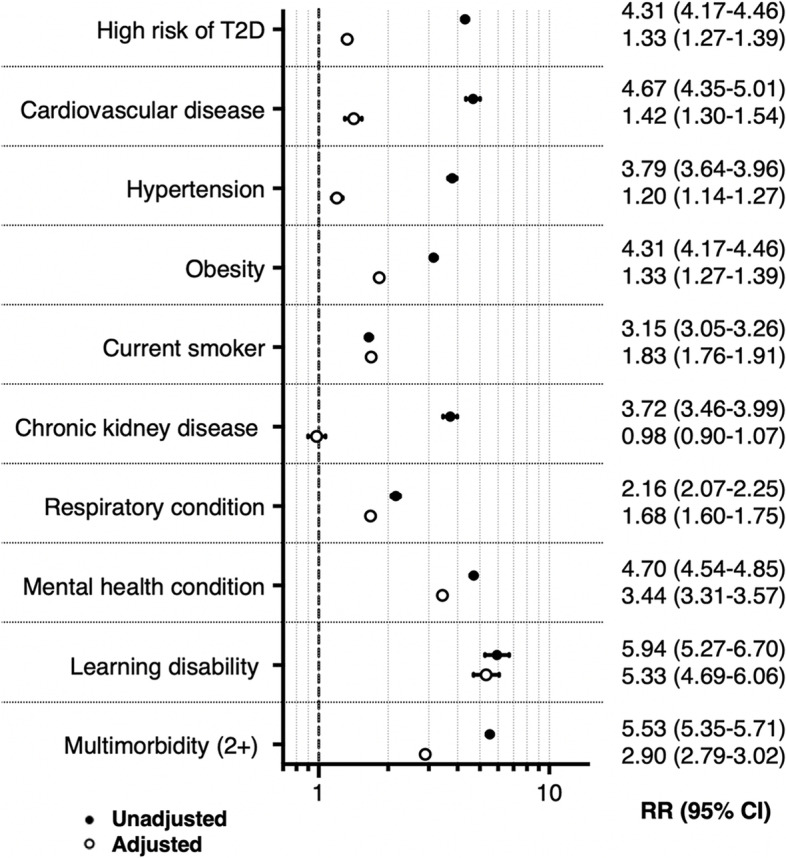
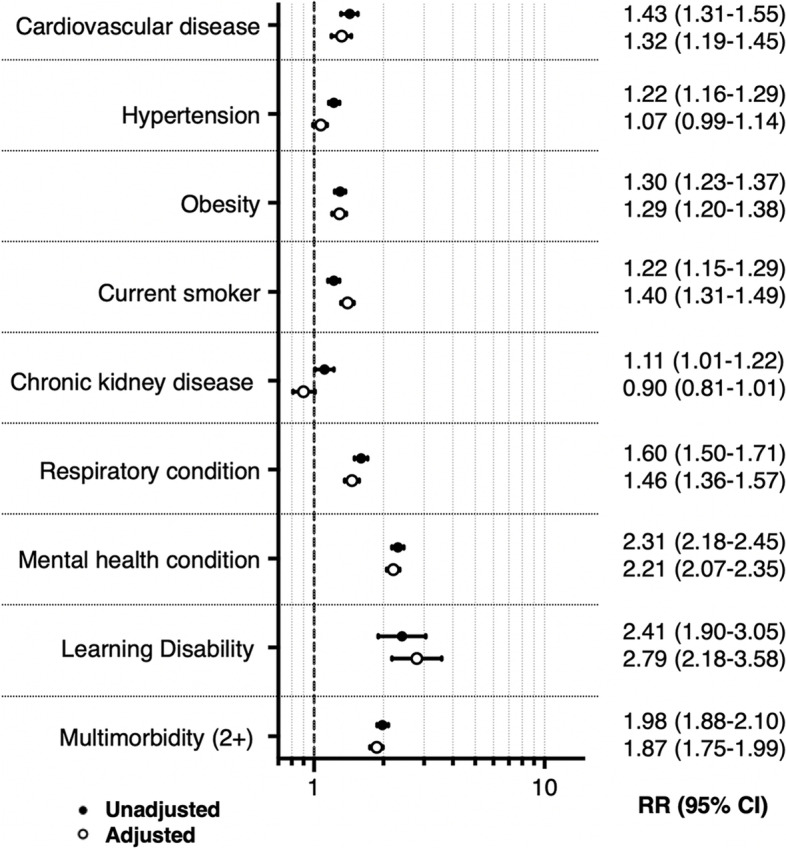
Results: People at high risk of T2D were four times more likely to be referred into SP than the eligible general population (RR 4.31 (95% CI 4.17-4.46)), with adjustment for socio-demographic variables resulting in attenuation (RR 1.33 (95% CI 1.27-1.39)). More people at risk of T2D were referred to SP than to NDPP, which could be explained by the broad referral criteria for SP and highly supportive (proactive, welcoming) environments. Holistic and sustained SP allowed acknowledgement of patients' wider socio-economic constraints and provision of long-term personalised care. The fact that SP was embedded within the local community and primary care infrastructure facilitated the timely exchange of information and cross-referrals across providers, resulting in enhanced service responsiveness.
Conclusions: Our study suggests that SP may offer an opportunity for individual-level T2D prevention to shift away from standardised, targeted and short-term strategies to approaches that are increasingly personalised, inclusive and long-term. Primary care-based SP seems most ideally placed to deliver such approaches where practitioners, providers and commissioners work collectively to achieve holistic, accessible, sustained and integrated services.
Keywords: Diabetes prevention; Health promotion; Primary care; Social prescribing.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Calderón-Larrañaga S, Braddick F. De la prescripción social a la recomendación de activos: ¿qué funciona, para quién, en qué contexto y cómo? FMC - Form Médica Contin en Atención Primaria. 2021;28(3):3–11. doi: 10.1016/j.fmc.2021.02.002. - DOI
-
- Hancock M. Keynote address. Social prescribing: coming of age. London: TheKing'sFund; 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
