

Myalgic Encephalomyelitis/Chronic Fatigue Syndrome is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic
- PMID: 36908615
- PMCID: PMC9998690
- DOI: 10.3389/fneur.2023.1090747
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic
Abstract
Background: The global prevalence of PASC is estimated to be present in 0·43 and based on the WHO estimation of 470 million worldwide COVID-19 infections, corresponds to around 200 million people experiencing long COVID symptoms. Despite this, its clinical features are not well-defined.
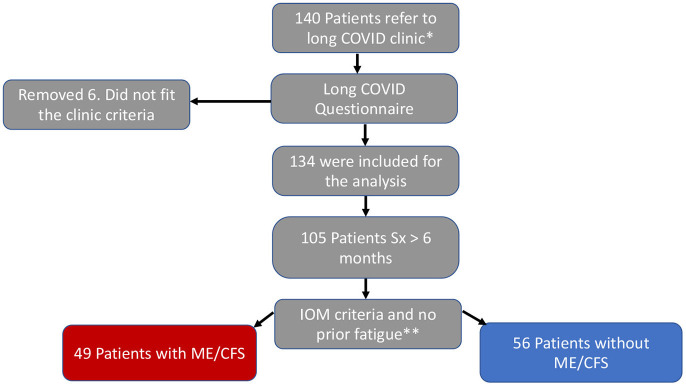
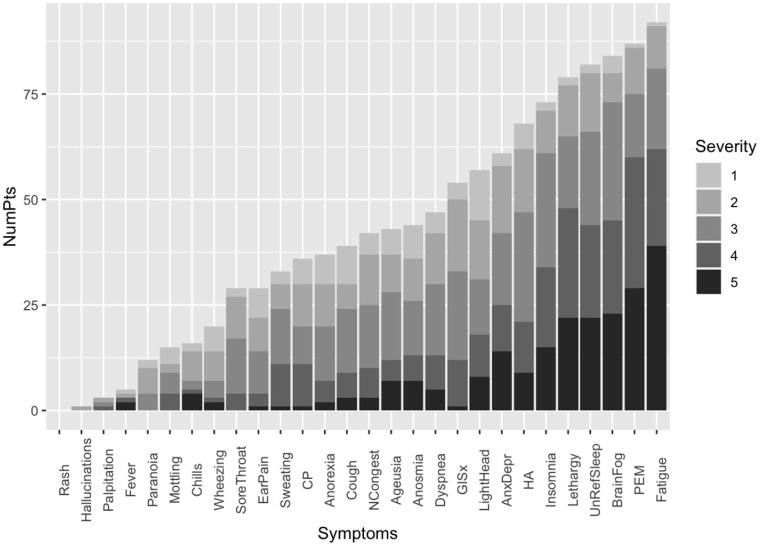
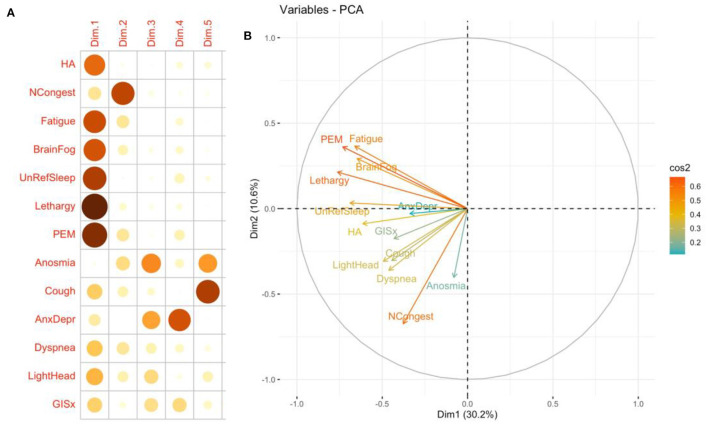
Methods: We collected retrospective data from 140 patients with PASC in a post-COVID-19 clinic on demographics, risk factors, illness severity (graded as one-mild to five-severe), functional status, and 29 symptoms and principal component symptoms cluster analysis. The Institute of Medicine (IOM) 2015 criteria were used to determine the Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) phenotype.
Findings: The median age was 47 years, 59.0% were female; 49.3% White, 17.2% Hispanic, 14.9% Asian, and 6.7% Black. Only 12.7% required hospitalization. Seventy-two (53.5%) patients had no known comorbid conditions. Forty-five (33.9%) were significantly debilitated. The median duration of symptoms was 285.5 days, and the number of symptoms was 12. The most common symptoms were fatigue (86.5%), post-exertional malaise (82.8%), brain fog (81.2%), unrefreshing sleep (76.7%), and lethargy (74.6%). Forty-three percent fit the criteria for ME/CFS, majority were female, and obesity (BMI > 30 Kg/m2) (P = 0.00377895) and worse functional status (P = 0.0110474) were significantly associated with ME/CFS.
Interpretations: Most PASC patients evaluated at our clinic had no comorbid condition and were not hospitalized for acute COVID-19. One-third of patients experienced a severe decline in their functional status. About 43% had the ME/CFS subtype.
Keywords: ME/CFS; PASC; post-COVID-19 clinic; prevalence; symptoms.
Copyright © 2023 Bonilla, Quach, Tiwari, Bonilla, Miglis, Yang, Eggert, Sharifi, Horomanski, Subramanian, Smirnoff, Simpson, Halawi, Sum-ping, Kalinowski, Patel, Shafer and Geng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Tenforde MW, Kim SS, Lindsell CJ, Billig Rose E, Shapiro NI, Files DC, et al. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a Multistate Health care systems network - United States, March-June 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:993–8. 10.15585/mmwr.mm6930e1 - DOI - PMC - PubMed
-
- CDC . Long COVID or Post-COVID Conditions. Atlanta, GA: CDC; (2022).
-
- COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. London: National Institute for Health and Care Excellence: Clinical Guidelines; (2020). - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous