

Case report: A case of acute disseminated encephalomyelitis after SARS-CoV-2 infection in pediatric patients
- PMID: 36908623
- PMCID: PMC9992531
- DOI: 10.3389/fneur.2023.1099458
Case report: A case of acute disseminated encephalomyelitis after SARS-CoV-2 infection in pediatric patients
Abstract
Introduction: Since the beginning, there has been enough evidence about the multi-systematic involvement of the coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Recent observations have revealed that, together with others, typical neurological manifestations are also associated with COVID-19 infection. In the first 2 years, children accounted for a few percent of cases, but with the emergence of the Omicron variant, the number of cases in the pediatric population has increased. It has been described that ~5% of the affected population suffered from severe neurological complications, such as seizure, coma, encephalitis, demyelinating disorders, and aseptic meningitis. Acute disseminated encephalomyelitis (ADEM) is an inflammatory demyelinating disease of the central nervous system. Typically, it presents in childhood and occurs 1 or 2 weeks after infection or vaccination.
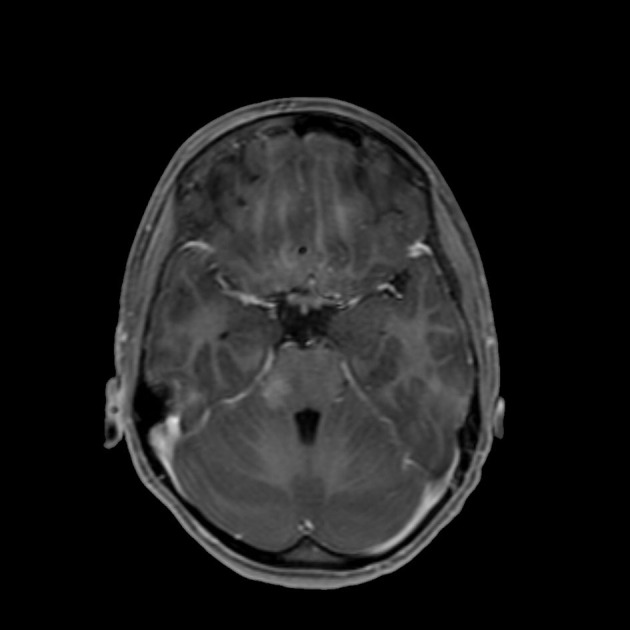
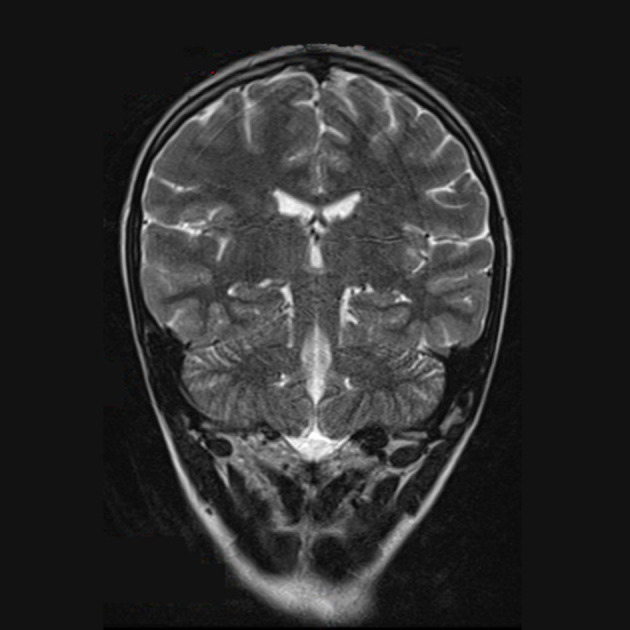
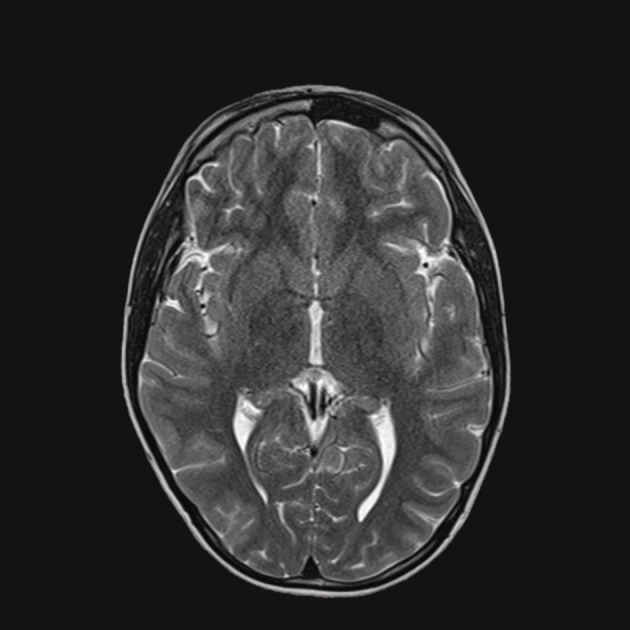
Case presentation: We present the case of a 12-year-old boy who developed ADEM, 10 days after an asymptomatic SARS-CoV-2 infection. Neurological symptoms began with headache, fever, irritability, paraplegia, and loss of sensitivity from the T1 level. The diagnosis of ADEM was confirmed by the typical signs found on brain MRI, whereas spinal cord MRI showed signs of transverse myelitis. The cerebrospinal fluid (CSF) testing excluded infections and did not reveal oligoclonal antibody bands (anti-MOG-negative and anti-AQP-negative). High-dose steroids (30 mg/kg/day) and IVIG (2 g/kg) were administered to the patient without any clinical improvement. The patient received a cycle of plasma exchange therapy, followed by rituximab infusion, with partial improvement. After 3 months, the magnetic resonance imaging (MRI) results demonstrated radiological improvement in accordance with the ADEM diagnosis.
Conclusion: This clinical case confirms that SARS-CoV-2 infections are increasingly implicated in severe neurological consequences in both adult and pediatric patients. While the most frequent complications that were reported in children included headache, altered mental status, and encephalopathy, ~5% of the individuals suffered from severe neurological complications, leading to lifelong sequelae. All physicians must be aware of these data and detect neurological signs of severe (or not) complications that require a specific follow-up and treatment.
Keywords: COVID-19; acute disseminated encephalopathy; children; complications; neurological complications.
Copyright © 2023 Cautilli, Feleppa, Valeriani, Papetti, Monte, Midulla and Spalice.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- UNICEF DATA ON LINE. Available online at: https://data.unicef.org/resources/covid-19-confirmed-cases-and-deaths-da... (accessed October 7, 2022).
-
- Ray STJ, Abdel-Mannan O, Sa M, Fuller C, Wood GK, Pysden K, et al. . Neurological manifestations of SARS-CoV-2 infection in hospitalised children and adolescents in the UK: a prospective national cohort study. Lancet Child Adolesc Health. (2021) 5:631–41. 10.1016/S2352-4642(21)00193-0 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous