

A Case Report of Iliopsoas Abscess Secondary to Small Bowel Fistula
- PMID: 36909091
- PMCID: PMC9998165
- DOI: 10.7759/cureus.34749
A Case Report of Iliopsoas Abscess Secondary to Small Bowel Fistula
Abstract
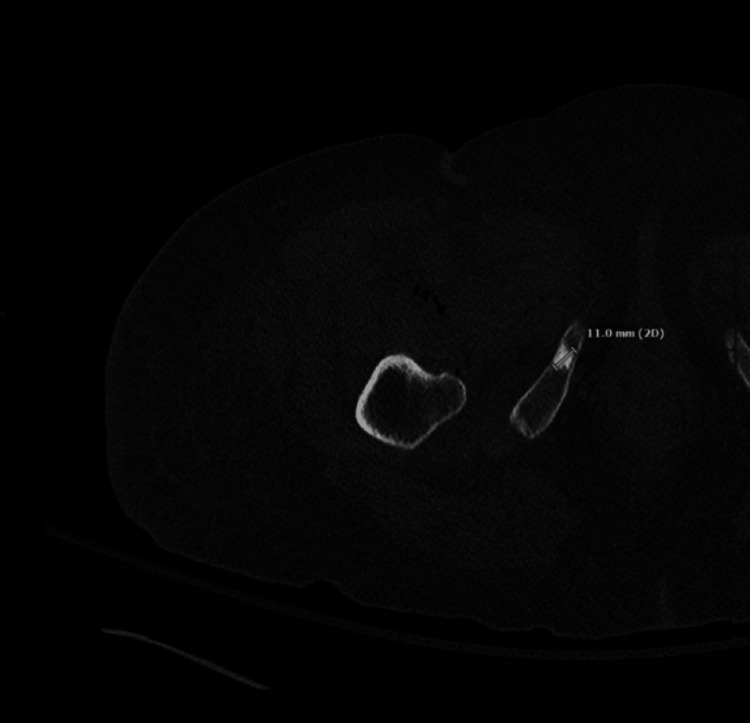
Iliopsoas abscesses (IPAs) are rare infections in the musculature that can be difficult to diagnose due to nonspecific presentations. These abscesses are most commonly caused by either the hematogenous spread of a separate infectious source in the body or secondary to Crohn's disease and are typically treated with antibiotic therapy and percutaneous drainage. For cases complicated by bowel disease, multiloculated psoas abscess, or gas-forming organisms, surgical drainage may be indicated. We present the case of an 81-year-old female with a history of colon cancer status post-cecum resection who presented with back pain, thigh pain, and constipation. Computerized tomography imaging showed concurrent small bowel obstruction and a right IPA extending down to the right thigh. Laparoscopic exploration revealed a small bowel fistulization to the right iliopsoas as the source of infection. Resection of the small bowel and surgical incision and drainage of the abscess were necessary for her treatment. The patient was discharged with vacuum-assisted closure of her wound after a hospital course complicated with chronic diarrhea. Bowel fistulization should be considered a potential cause of IPAs in patients with a complicated gastrointestinal history.
Keywords: atypical back pain; fistulization; iliopsoas abscess; incision and drainage of abscess; small bowel obstruction.
Copyright © 2023, Guerrero et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Microbiology and outcome of iliopsoas abscess in 124 patients. López VN, Ramos JM, Meseguer V, et al. Medicine (Baltimore) 2009;88:120–130. - PubMed
-
- Pyogenic psoas abscess: worldwide variations in etiology. Ricci MA, Rose FB, Meyer KK. World J Surg. 1986;10:834–843. - PubMed
-
- Psoas abscess: making an early diagnosis in the ED. Chern CH, Hu SC, Kao WF, Tsai J, Yen D, Lee CH. Am J Emerg Med. 1997;15:83–88. - PubMed
-
- Psoas abscess secondary to discitis: a case report of conservative management. Qureshi NH, O'Brien DP, Allcutt DA. J Spinal Disord. 2000;13:73–76. - PubMed
Publication types
LinkOut - more resources
Full Text Sources