

This is a preprint.
REPRODUCIBLE AND CLINICALLY TRANSLATABLE DEEP NEURAL NETWORKS FOR CANCER SCREENING
- PMID: 36909463
- PMCID: PMC10002800
- DOI: 10.21203/rs.3.rs-2526701/v1
REPRODUCIBLE AND CLINICALLY TRANSLATABLE DEEP NEURAL NETWORKS FOR CANCER SCREENING
Update in
-
Reproducible and clinically translatable deep neural networks for cervical screening.Sci Rep. 2023 Dec 8;13(1):21772. doi: 10.1038/s41598-023-48721-1. Sci Rep. 2023. PMID: 38066031 Free PMC article.
Abstract
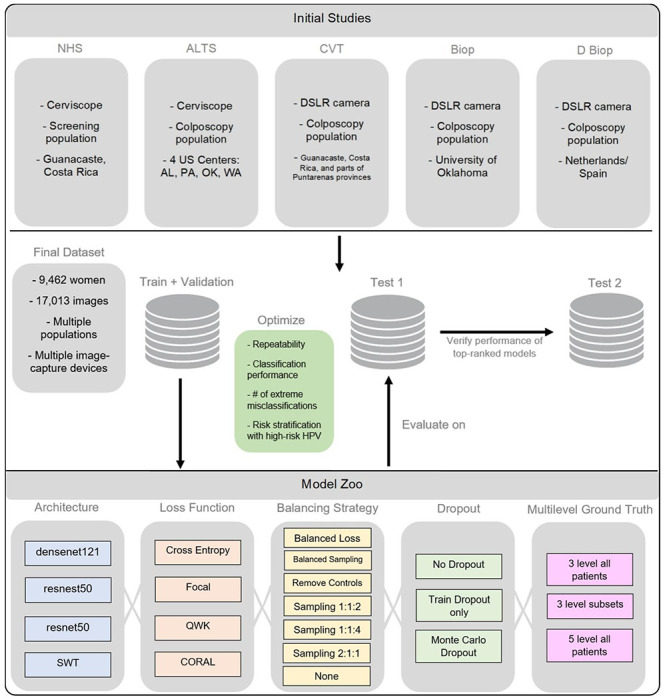
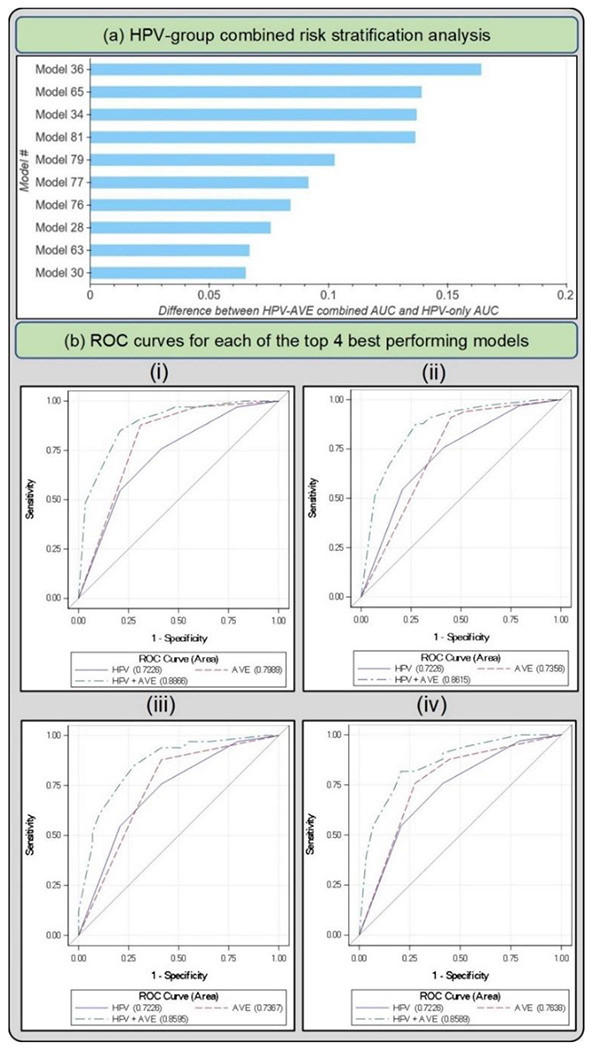
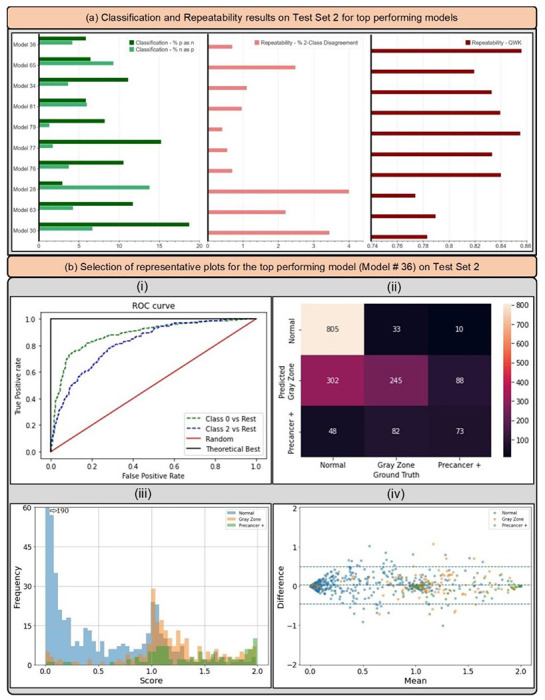
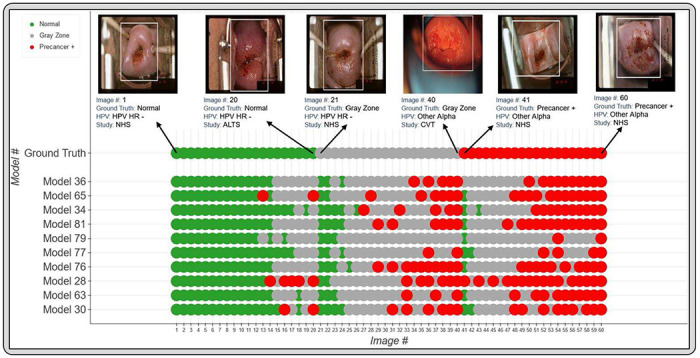
Cervical cancer is a leading cause of cancer mortality, with approximately 90% of the 250,000 deaths per year occurring in low- and middle-income countries (LMIC). Secondary prevention with cervical screening involves detecting and treating precursor lesions; however, scaling screening efforts in LMIC has been hampered by infrastructure and cost constraints. Recent work has supported the development of an artificial intelligence (AI) pipeline on digital images of the cervix to achieve an accurate and reliable diagnosis of treatable precancerous lesions. In particular, WHO guidelines emphasize visual triage of women testing positive for human papillomavirus (HPV) as the primary screen, and AI could assist in this triage task. Published AI reports have exhibited overfitting, lack of portability, and unrealistic, near-perfect performance estimates. To surmount recognized issues, we implemented a comprehensive deep-learning model selection and optimization study on a large, collated, multi-institutional dataset of 9,462 women (17,013 images). We evaluated relative portability, repeatability, and classification performance. The top performing model, when combined with HPV type, achieved an area under the Receiver Operating Characteristics (ROC) curve (AUC) of 0.89 within our study population of interest, and a limited total extreme misclassification rate of 3.4%, on held-aside test sets. Our work is among the first efforts at designing a robust, repeatable, accurate and clinically translatable deep-learning model for cervical screening.
Keywords: artificial intelligence; cervical cancer screening; deep learning; human papillomavirus.
Conflict of interest statement
Additional Declarations: There is NO Competing Interest.
Figures
References
-
- Piccialli F, Somma V Di, Giampaolo F, Cuomo S, Fortino G. A survey on deep learning in medicine: Why, how and when? Inf Fusion. 2021. Feb 1 ;66:111–37.
-
- Sperr E. PubMed by Year [Internet], [cited 2022 Nov 12]. Available from: https://esperr.github.io/pubmed-by-year/?q1=%22deeplearning%22or%22neura...
-
- Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, Blau HM, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nat 2017 5427639 [Internet]. 2017. Jan 25 [cited 2022 Nov 12];542(7639):115–8. Available from: https://www.nature.com/articles/nature21056 - PMC - PubMed
-
- Hannun AY, Rajpurkar P, Haghpanahi M, Tison GH, Bourn C, Turakhia MP, et al. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat Med 2019 251 [Internet]. 2019. Jan 7 [cited 2022 Nov 12];25(1):65–9. Available from: https://www.nature.com/articles/s41591-018-0268-3 - PMC - PubMed
-
- Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med 2019 251 [Internet]. 2019. Jan 7 [cited 2022 May 5];25(1):44–56. Available from: https://www.nature.com/articles/s41591-018-0300-7 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
