

Advanced MR Techniques for Preoperative Glioma Characterization: Part 2
- PMID: 36912262
- PMCID: PMC10947037
- DOI: 10.1002/jmri.28663
Advanced MR Techniques for Preoperative Glioma Characterization: Part 2
Erratum in
-
Erratum to "Advanced MR Techniques for Preoperative Glioma Characterization: Part 2".J Magn Reson Imaging. 2024 Apr;59(4):1468. doi: 10.1002/jmri.28934. Epub 2023 Aug 11. J Magn Reson Imaging. 2024. PMID: 37565520 Free PMC article. No abstract available.
Abstract
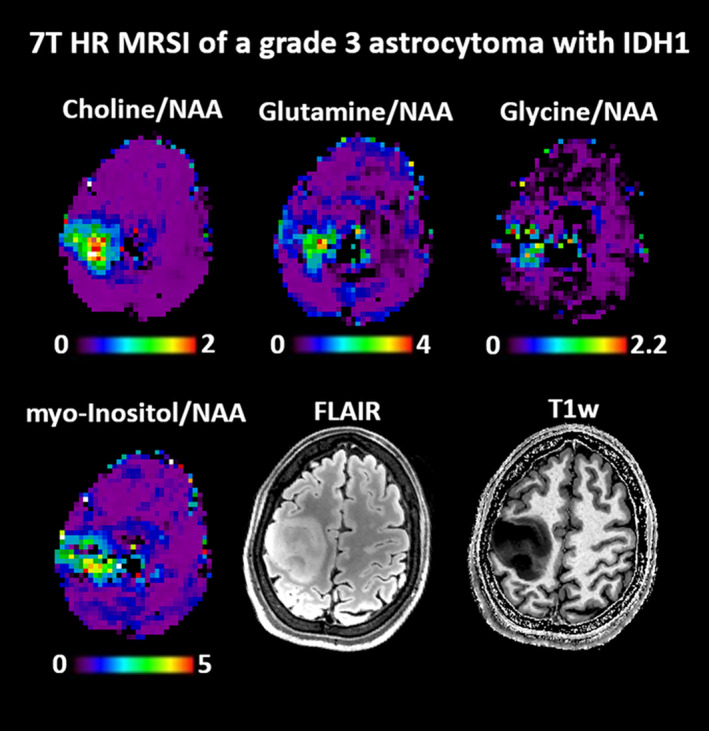
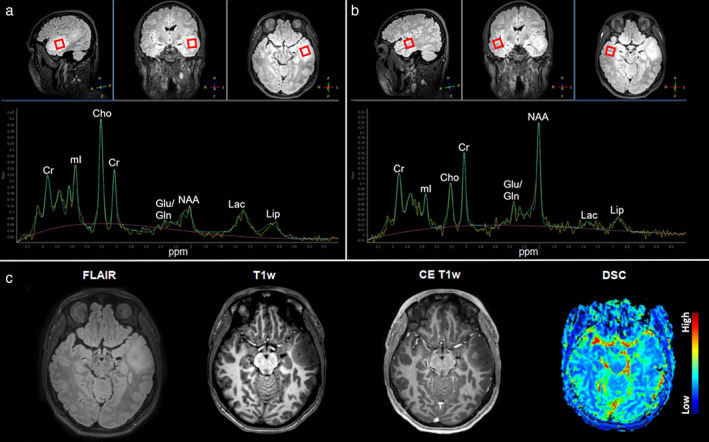
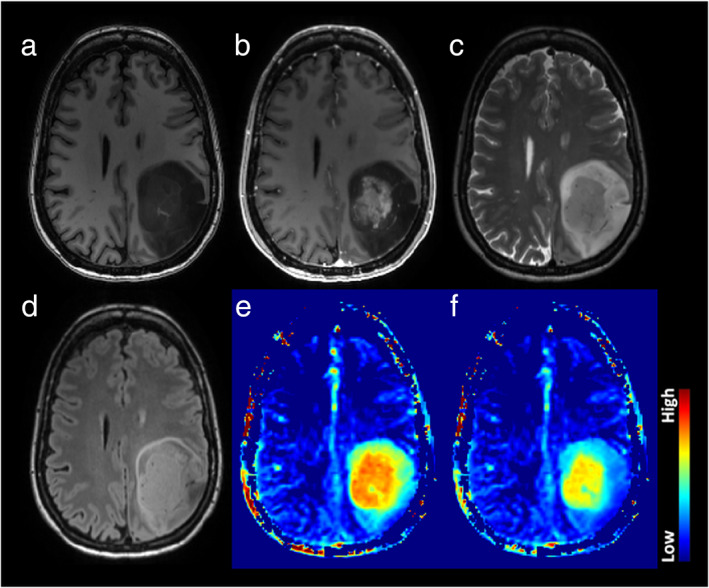
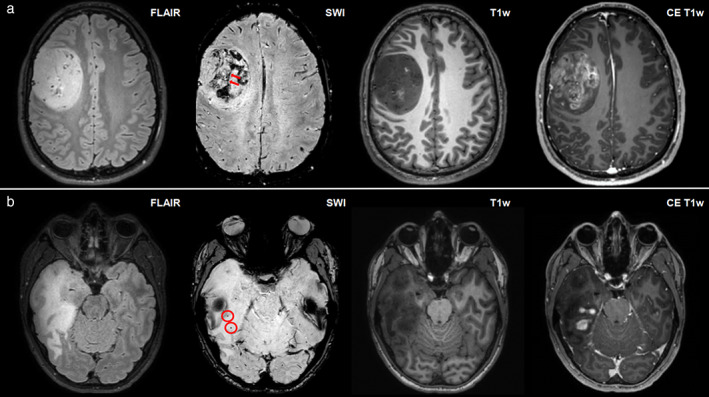
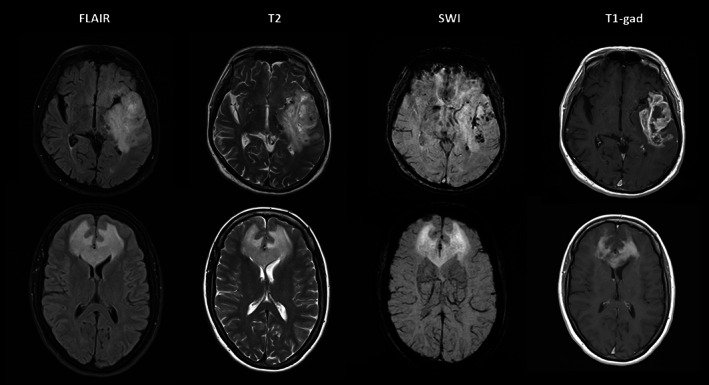
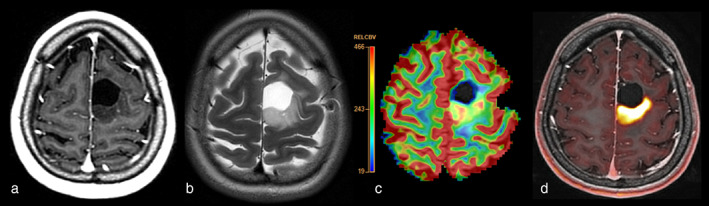
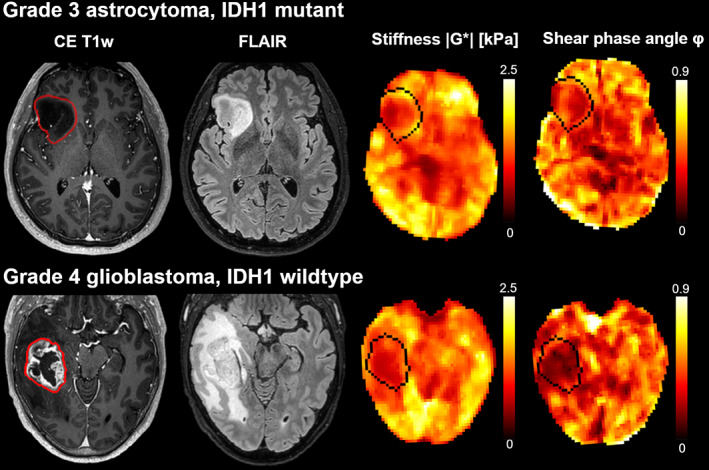
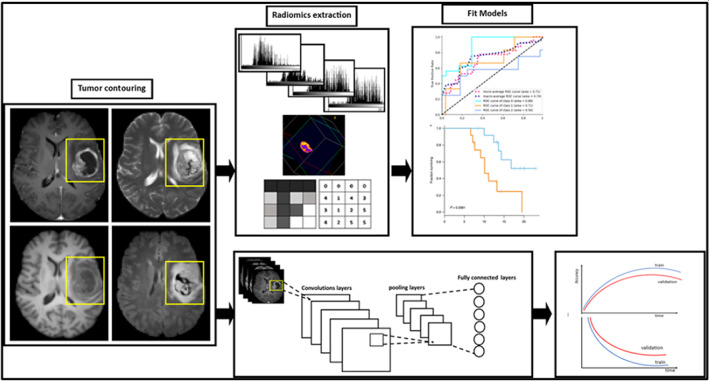
Preoperative clinical MRI protocols for gliomas, brain tumors with dismal outcomes due to their infiltrative properties, still rely on conventional structural MRI, which does not deliver information on tumor genotype and is limited in the delineation of diffuse gliomas. The GliMR COST action wants to raise awareness about the state of the art of advanced MRI techniques in gliomas and their possible clinical translation. This review describes current methods, limits, and applications of advanced MRI for the preoperative assessment of glioma, summarizing the level of clinical validation of different techniques. In this second part, we review magnetic resonance spectroscopy (MRS), chemical exchange saturation transfer (CEST), susceptibility-weighted imaging (SWI), MRI-PET, MR elastography (MRE), and MR-based radiomics applications. The first part of this review addresses dynamic susceptibility contrast (DSC) and dynamic contrast-enhanced (DCE) MRI, arterial spin labeling (ASL), diffusion-weighted MRI, vessel imaging, and magnetic resonance fingerprinting (MRF). EVIDENCE LEVEL: 3. TECHNICAL EFFICACY: Stage 2.
Keywords: GliMR 2.0; brain; contrasts; glioma; level of clinical validation; preoperative.
© 2023 The Authors. Journal of Magnetic Resonance Imaging published by Wiley Periodicals LLC on behalf of International Society for Magnetic Resonance in Medicine.
Figures
References
-
- Sanai N, Berger MS. Surgical oncology for gliomas: The state of the art. Nat Rev Clin Oncol 2018;15:112‐125. - PubMed
-
- Smits M. MRI biomarkers in neuro‐oncology. Nat Rev Neurol 2021;17:486‐500. - PubMed
-
- Booth TC, Wiegers EC, Warnert EAH, et al. High‐grade glioma treatment response monitoring biomarkers: A position statement on the evidence supporting the use of advanced MRI techniques in the clinic, and the latest bench‐to‐bedside developments. Part 2: Spectroscopy, chemical exchange saturation, multiparametric imaging, and radiomics. Front Oncol 2021;11:811425. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
