

Diagnostic Accuracy of Portable, Handheld Point-of-Care Tests vs Laboratory-Based Bilirubin Quantification in Neonates: A Systematic Review and Meta-analysis
- PMID: 36912856
- PMCID: PMC10012043
- DOI: 10.1001/jamapediatrics.2023.0059
Diagnostic Accuracy of Portable, Handheld Point-of-Care Tests vs Laboratory-Based Bilirubin Quantification in Neonates: A Systematic Review and Meta-analysis
Abstract
Importance: Quantification of bilirubin in blood is essential for early diagnosis and timely treatment of neonatal hyperbilirubinemia. Handheld point-of-care (POC) devices may overcome the current issues with conventional laboratory-based bilirubin (LBB) quantification.
Objective: To systematically evaluate the reported diagnostic accuracy of POC devices compared with LBB quantification.
Data sources: A systematic literature search was conducted in 6 electronic databases (Ovid MEDLINE, Embase, Web of Science Core Collection, Cochrane Central Register of Controlled Trials, CINAHL, and Google Scholar) up to December 5, 2022.
Study selection: Studies were included in this systematic review and meta-analysis if they had a prospective cohort, retrospective cohort, or cross-sectional design and reported on the comparison between POC device(s) and LBB quantification in neonates aged 0 to 28 days. Point-of-care devices needed the following characteristics: portable, handheld, and able to provide a result within 30 minutes. This study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses reporting guideline.
Data extraction and synthesis: Data extraction was performed by 2 independent reviewers into a prespecified, customized form. Risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies 2 tool. Meta-analysis was performed of multiple Bland-Altman studies using the Tipton and Shuster method for the main outcome.
Main outcomes and measures: The main outcome was mean difference and limits of agreement in bilirubin levels between POC device and LBB quantification. Secondary outcomes were (1) turnaround time (TAT), (2) blood volumes, and (3) percentage of failed quantifications.
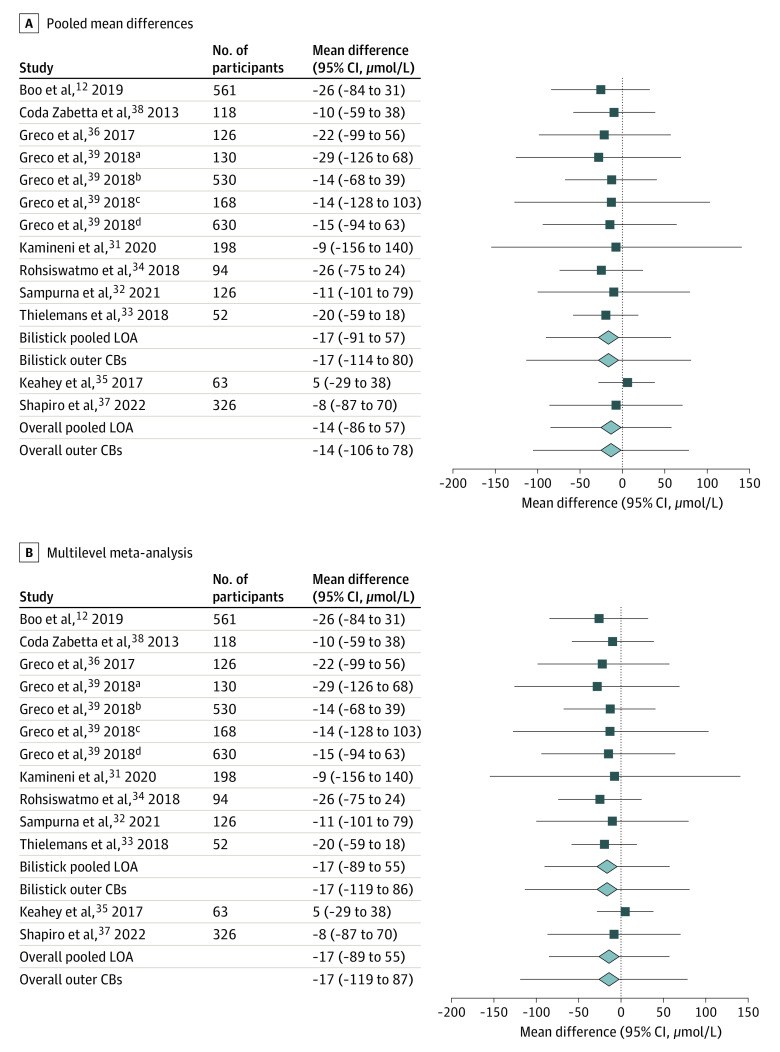
Results: Ten studies met the inclusion criteria (9 cross-sectional studies and 1 prospective cohort study), representing 3122 neonates. Three studies were considered to have a high risk of bias. The Bilistick was evaluated as the index test in 8 studies and the BiliSpec in 2. A total of 3122 paired measurements showed a pooled mean difference in total bilirubin levels of -14 μmol/L, with pooled 95% CBs of -106 to 78 μmol/L. For the Bilistick, the pooled mean difference was -17 μmol/L (95% CBs, -114 to 80 μmol/L). Point-of-care devices were faster in returning results compared with LBB quantification, whereas blood volume needed was less. The Bilistick was more likely to have a failed quantification compared with LBB.
Conclusions and relevance: Despite the advantages that handheld POC devices offer, these findings suggest that the imprecision for measurement of neonatal bilirubin needs improvement to tailor neonatal jaundice management.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
