

Proactive Contact Tracing
- PMID: 36913342
- PMCID: PMC10010527
- DOI: 10.1371/journal.pdig.0000199
Proactive Contact Tracing
Abstract
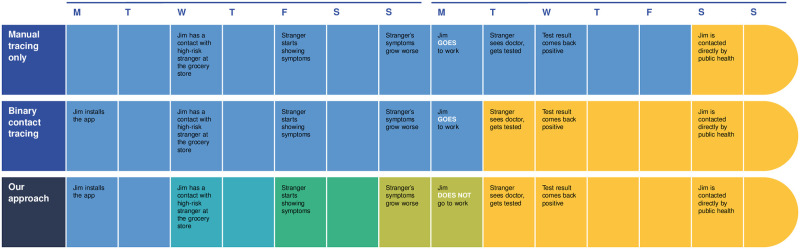
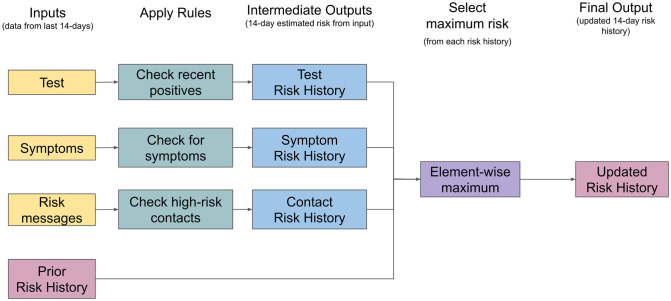
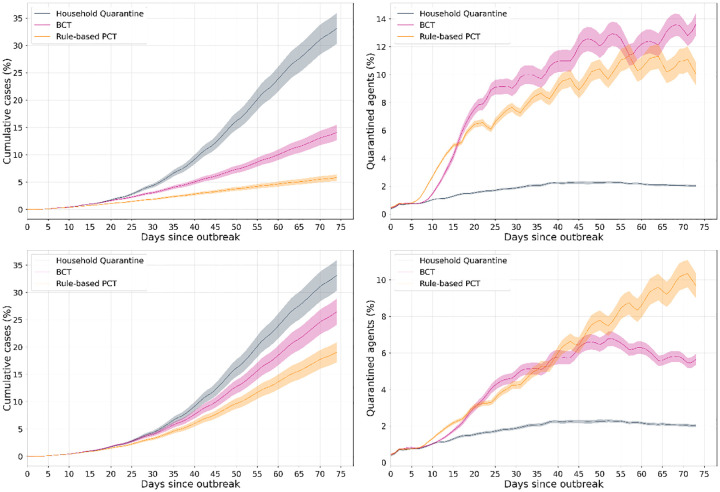
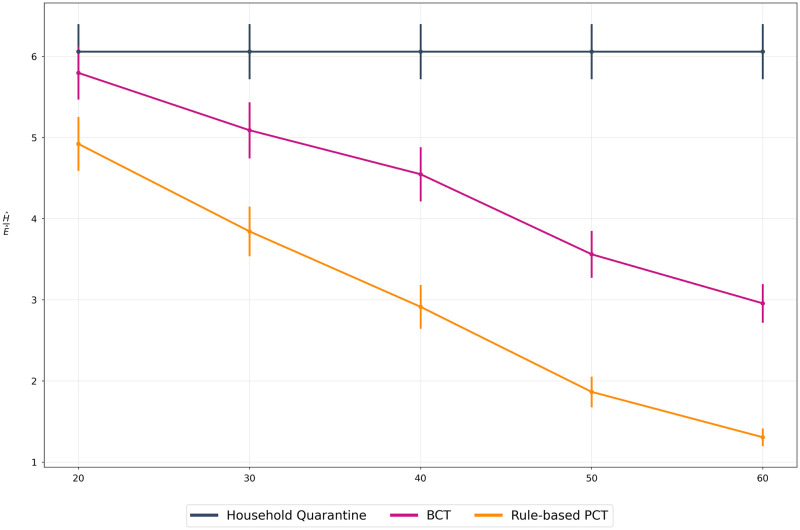
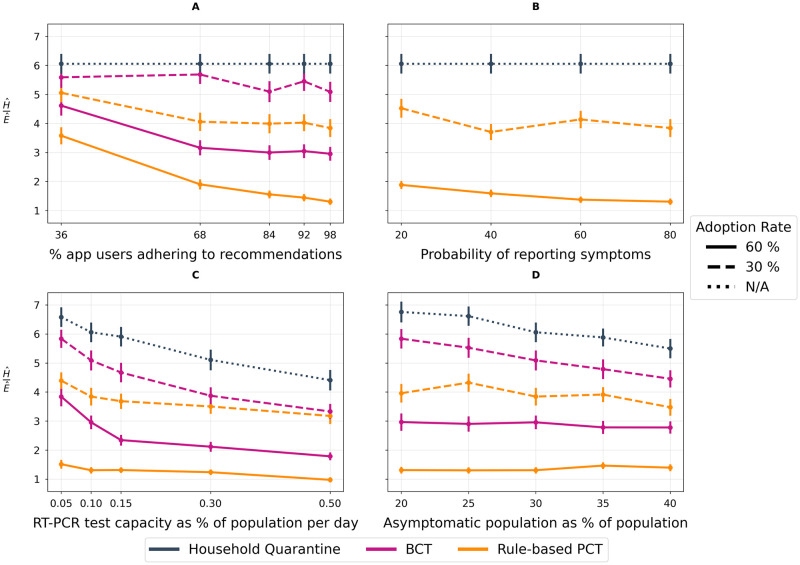
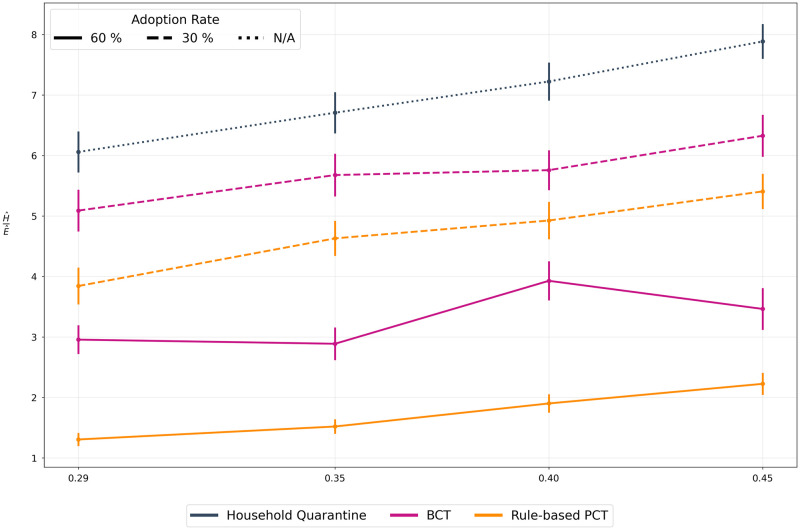
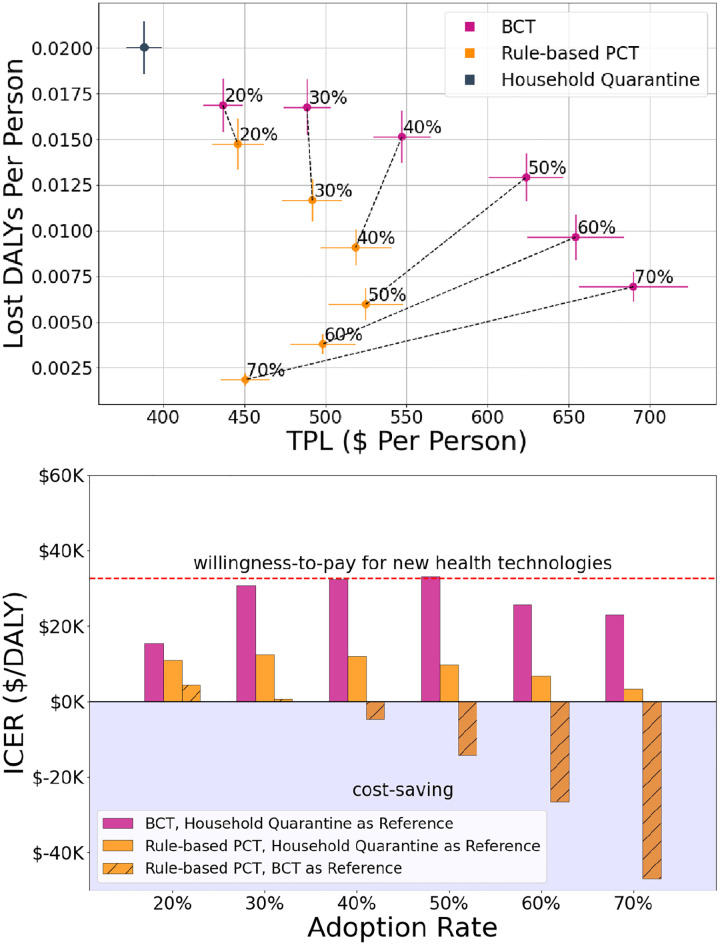
The COVID-19 pandemic has spurred an unprecedented demand for interventions that can reduce disease spread without excessively restricting daily activity, given negative impacts on mental health and economic outcomes. Digital contact tracing (DCT) apps have emerged as a component of the epidemic management toolkit. Existing DCT apps typically recommend quarantine to all digitally-recorded contacts of test-confirmed cases. Over-reliance on testing may, however, impede the effectiveness of such apps, since by the time cases are confirmed through testing, onward transmissions are likely to have occurred. Furthermore, most cases are infectious over a short period; only a subset of their contacts are likely to become infected. These apps do not fully utilize data sources to base their predictions of transmission risk during an encounter, leading to recommendations of quarantine to many uninfected people and associated slowdowns in economic activity. This phenomenon, commonly termed as "pingdemic," may additionally contribute to reduced compliance to public health measures. In this work, we propose a novel DCT framework, Proactive Contact Tracing (PCT), which uses multiple sources of information (e.g. self-reported symptoms, received messages from contacts) to estimate app users' infectiousness histories and provide behavioral recommendations. PCT methods are by design proactive, predicting spread before it occurs. We present an interpretable instance of this framework, the Rule-based PCT algorithm, designed via a multi-disciplinary collaboration among epidemiologists, computer scientists, and behavior experts. Finally, we develop an agent-based model that allows us to compare different DCT methods and evaluate their performance in negotiating the trade-off between epidemic control and restricting population mobility. Performing extensive sensitivity analysis across user behavior, public health policy, and virological parameters, we compare Rule-based PCT to i) binary contact tracing (BCT), which exclusively relies on test results and recommends a fixed-duration quarantine, and ii) household quarantine (HQ). Our results suggest that both BCT and Rule-based PCT improve upon HQ, however, Rule-based PCT is more efficient at controlling spread of disease than BCT across a range of scenarios. In terms of cost-effectiveness, we show that Rule-based PCT pareto-dominates BCT, as demonstrated by a decrease in Disability Adjusted Life Years, as well as Temporary Productivity Loss. Overall, we find that Rule-based PCT outperforms existing approaches across a varying range of parameters. By leveraging anonymized infectiousness estimates received from digitally-recorded contacts, PCT is able to notify potentially infected users earlier than BCT methods and prevent onward transmissions. Our results suggest that PCT-based applications could be a useful tool in managing future epidemics.
Copyright: © 2023 Gupta et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
LinkOut - more resources
Full Text Sources