

Optimal dietary patterns for prevention of chronic disease
- PMID: 36914892
- PMCID: PMC10294543
- DOI: 10.1038/s41591-023-02235-5
Optimal dietary patterns for prevention of chronic disease
Erratum in
-
Author Correction: Optimal dietary patterns for prevention of chronic disease.Nat Med. 2024 Jun;30(6):1786. doi: 10.1038/s41591-024-02889-9. Nat Med. 2024. PMID: 38454128 No abstract available.
Abstract
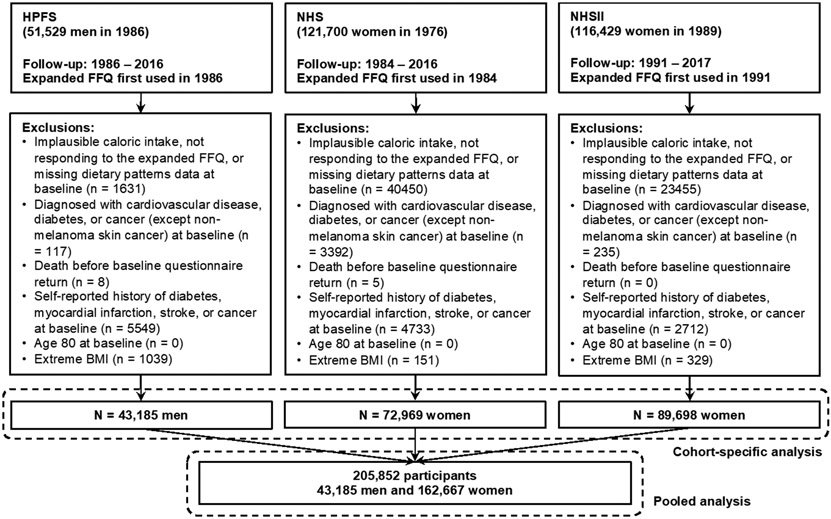
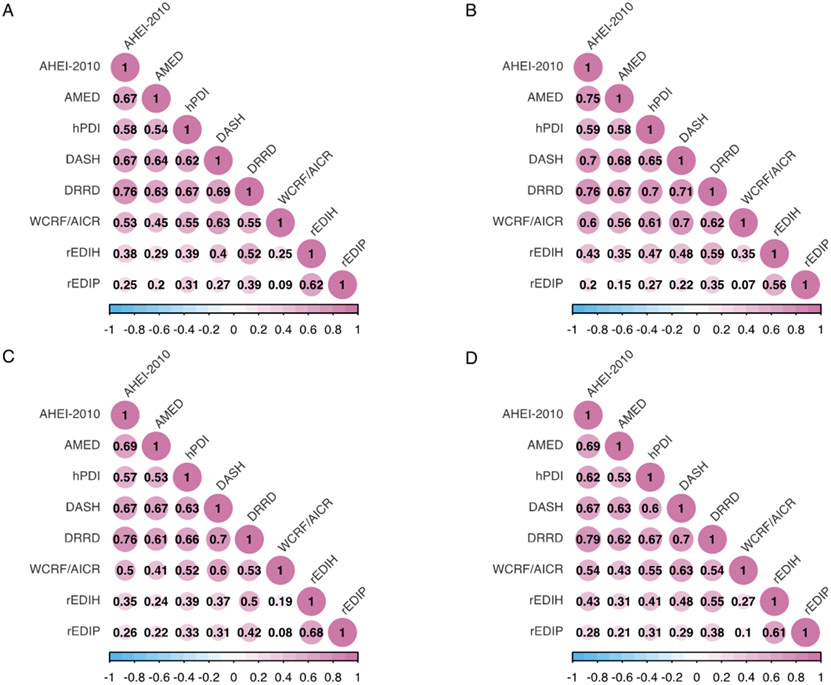
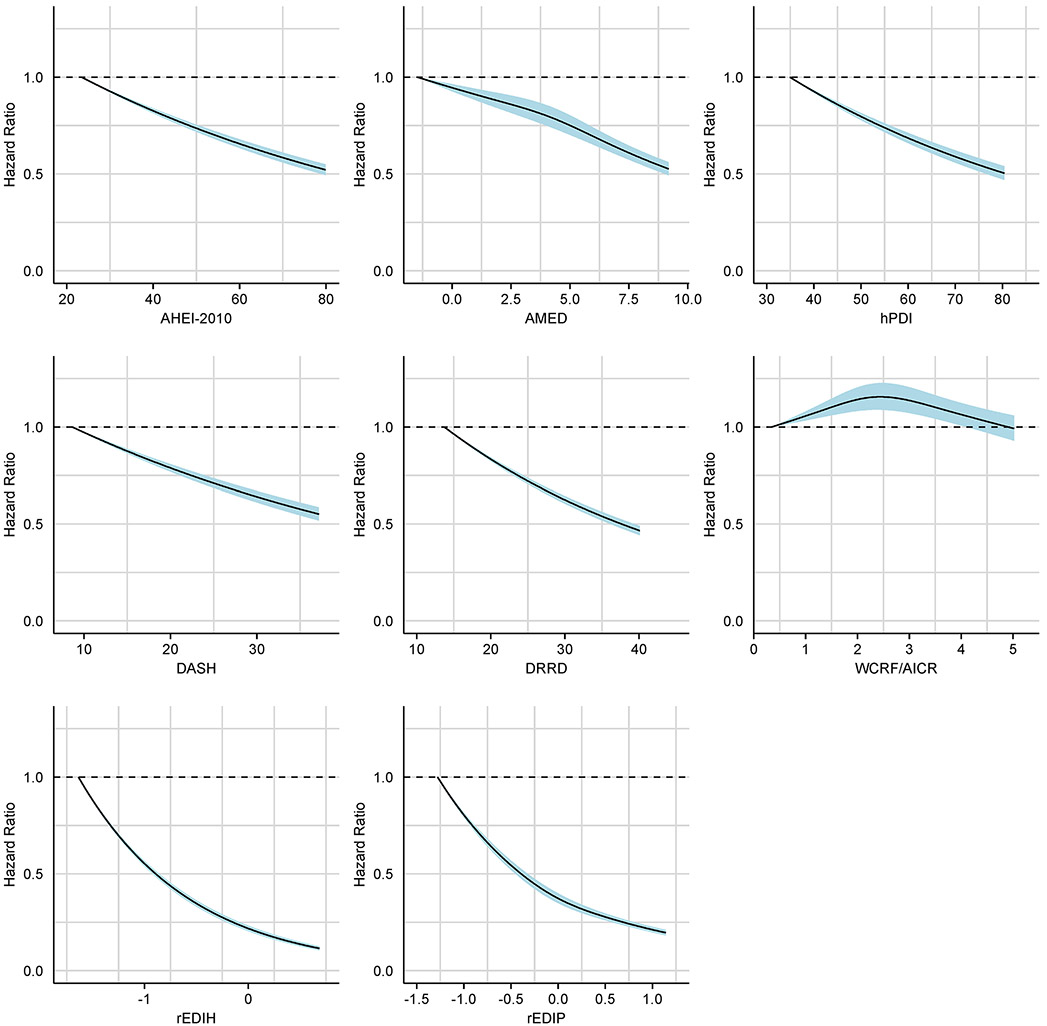
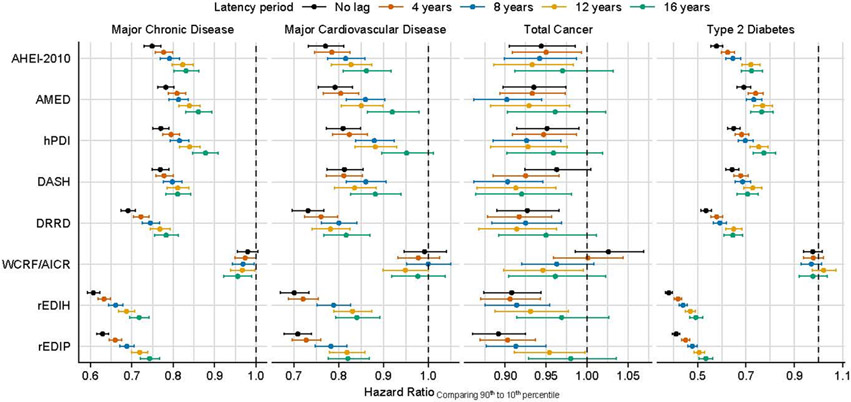
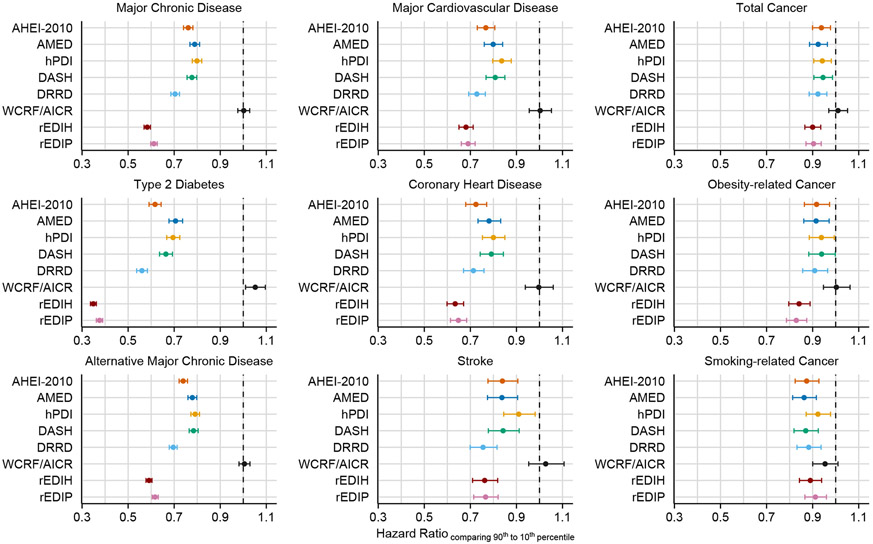
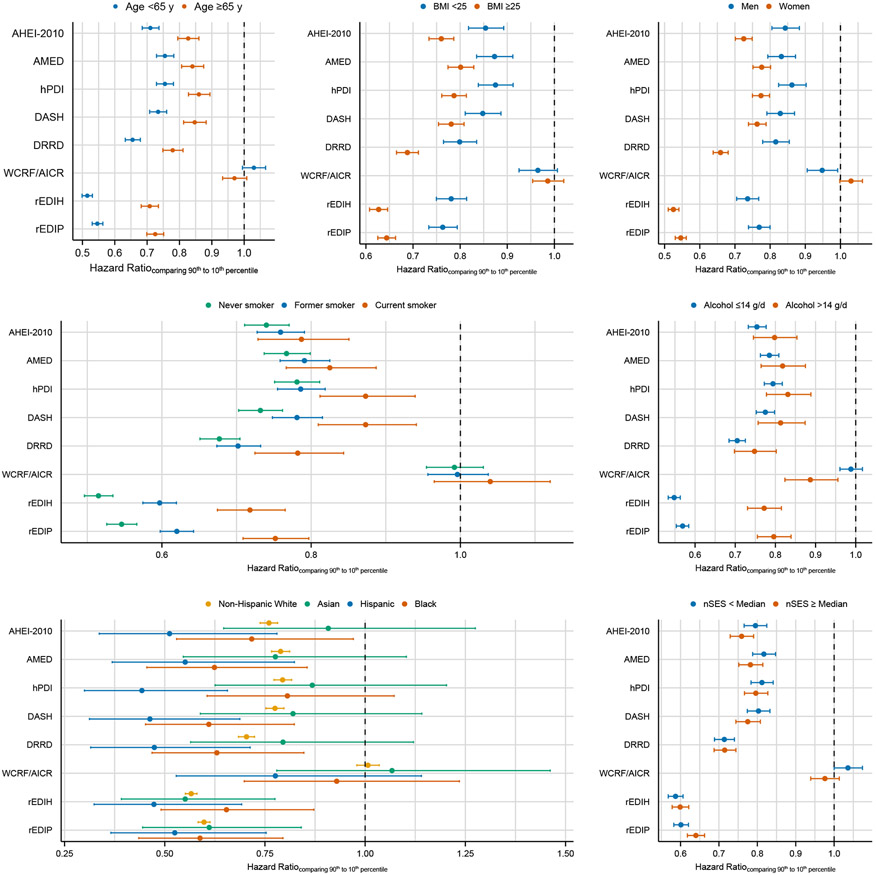
Multiple dietary patterns have been associated with different diseases; however, their comparability to improve overall health has yet to be determined. Here, in 205,852 healthcare professionals from three US cohorts followed for up to 32 years, we prospectively assessed two mechanism-based diets and six diets based on dietary recommendations in relation to major chronic disease, defined as a composite outcome of incident major cardiovascular disease (CVD), type 2 diabetes and cancer. We demonstrated that adherence to a healthy diet was generally associated with a lower risk of major chronic disease (hazard ratio (HR) comparing the 90th with the 10th percentile of dietary pattern scores = 0.58-0.80). Participants with low insulinemic (HR = 0.58, 95% confidence interval (CI) = 0.57, 0.60), low inflammatory (HR = 0.61, 95% CI = 0.60, 0.63) or diabetes risk-reducing (HR = 0.70, 95% CI = 0.69, 0.72) diet had the largest risk reduction for incident major CVD, type 2 diabetes and cancer as a composite and individually. Similar findings were observed across gender and diverse ethnic groups. Our results suggest that dietary patterns associated with markers of hyperinsulinemia and inflammation and diabetes development may inform on future dietary guidelines for chronic disease prevention.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing Interests
The authors have declared that no conflict of interest exists.
Figures
References
-
- Buttorff C, Ruder T & Bauman M Multiple Chronic Conditions in the United States. (RAND Corporation, Santa Monica, CA, 2017).
-
- Murphy SL, Kochanek KD, Xu J & Arias E Mortality in the United States, 2020. NCHS Data Brief, 1–8 (2021). - PubMed
-
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019. May 11;393(10184):1958–1972. doi: 10.1016/S0140-6736(19)30041-8. Epub 2019 Apr 4. Erratum in: Lancet. 2021 Jun 26;397(10293):2466. PMID: 30954305; PMCID: PMC6899507. - DOI - PMC - PubMed
-
- Dietary Guidelines Advisory Committee. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services. (U.S. Department of Agriculture, Agricultural Research Service, Washington, D.C., 2020).
Methods only references
-
- Salvini S, et al. Food-based validation of a dietary questionnaire: the effects of week-to-week variation in food consumption. Int J Epidemiol 18, 858–867 (1989). - PubMed
-
- Feskanich D, et al. Reproducibility and validity of food intake measurements from a semiquantitative food frequency questionnaire. J Am Diet Assoc 93, 790–796 (1993). - PubMed
-
- Hu FB, et al. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am J Clin Nutr 69, 243–249 (1999). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
