

A non-antibiotic-disrupted gut microbiome is associated with clinical responses to CD19-CAR-T cell cancer immunotherapy
- PMID: 36914893
- PMCID: PMC10121864
- DOI: 10.1038/s41591-023-02234-6
A non-antibiotic-disrupted gut microbiome is associated with clinical responses to CD19-CAR-T cell cancer immunotherapy
Abstract
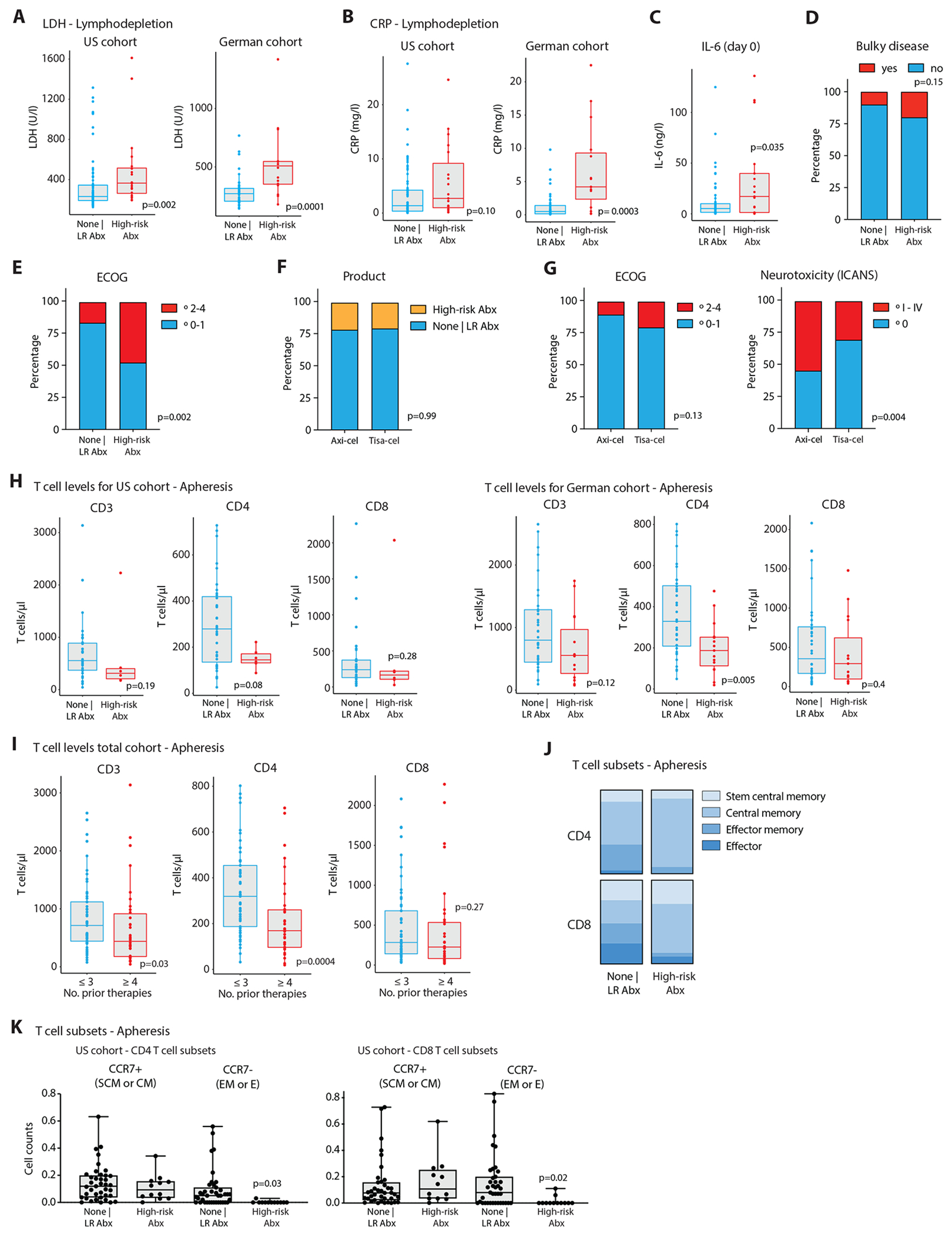
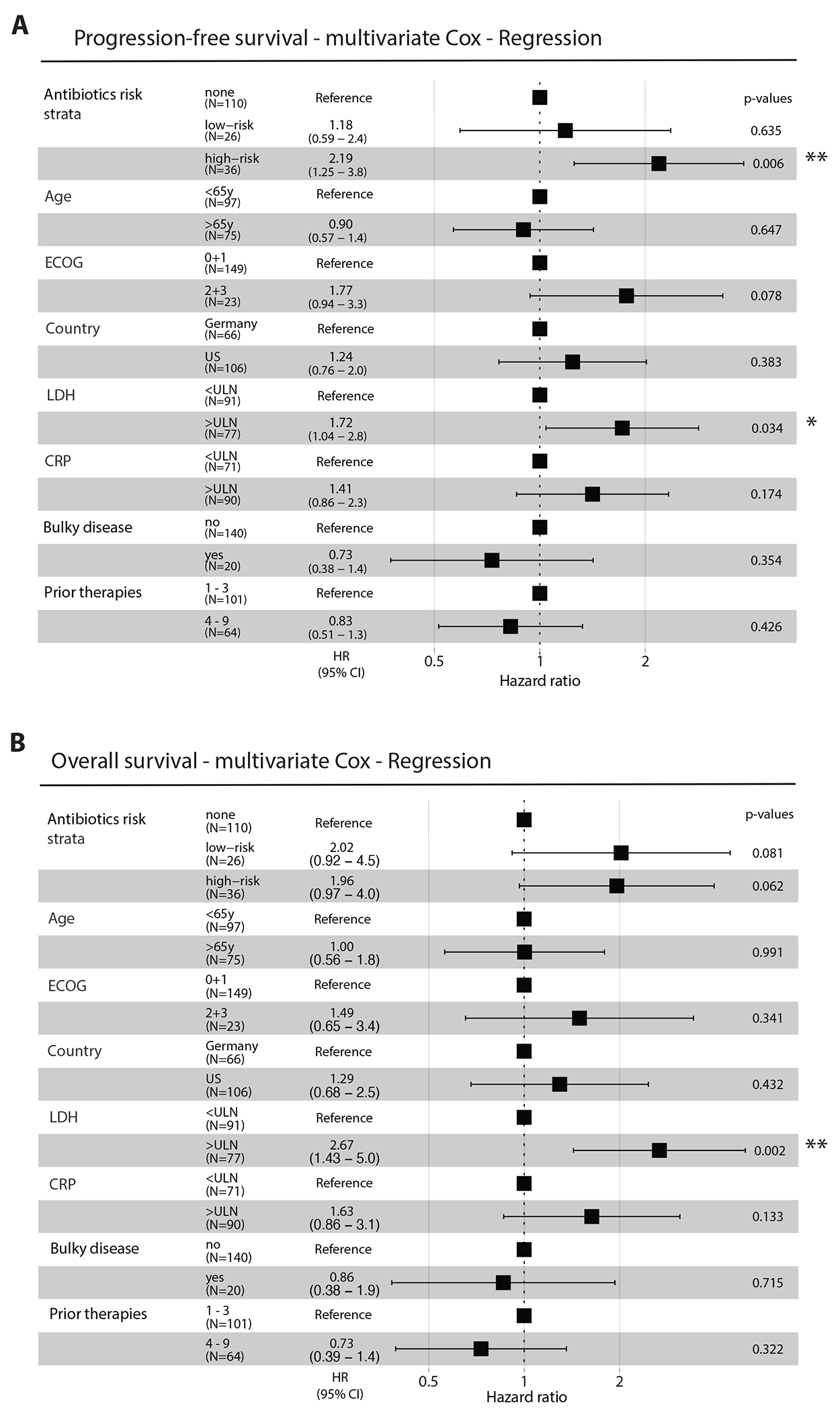
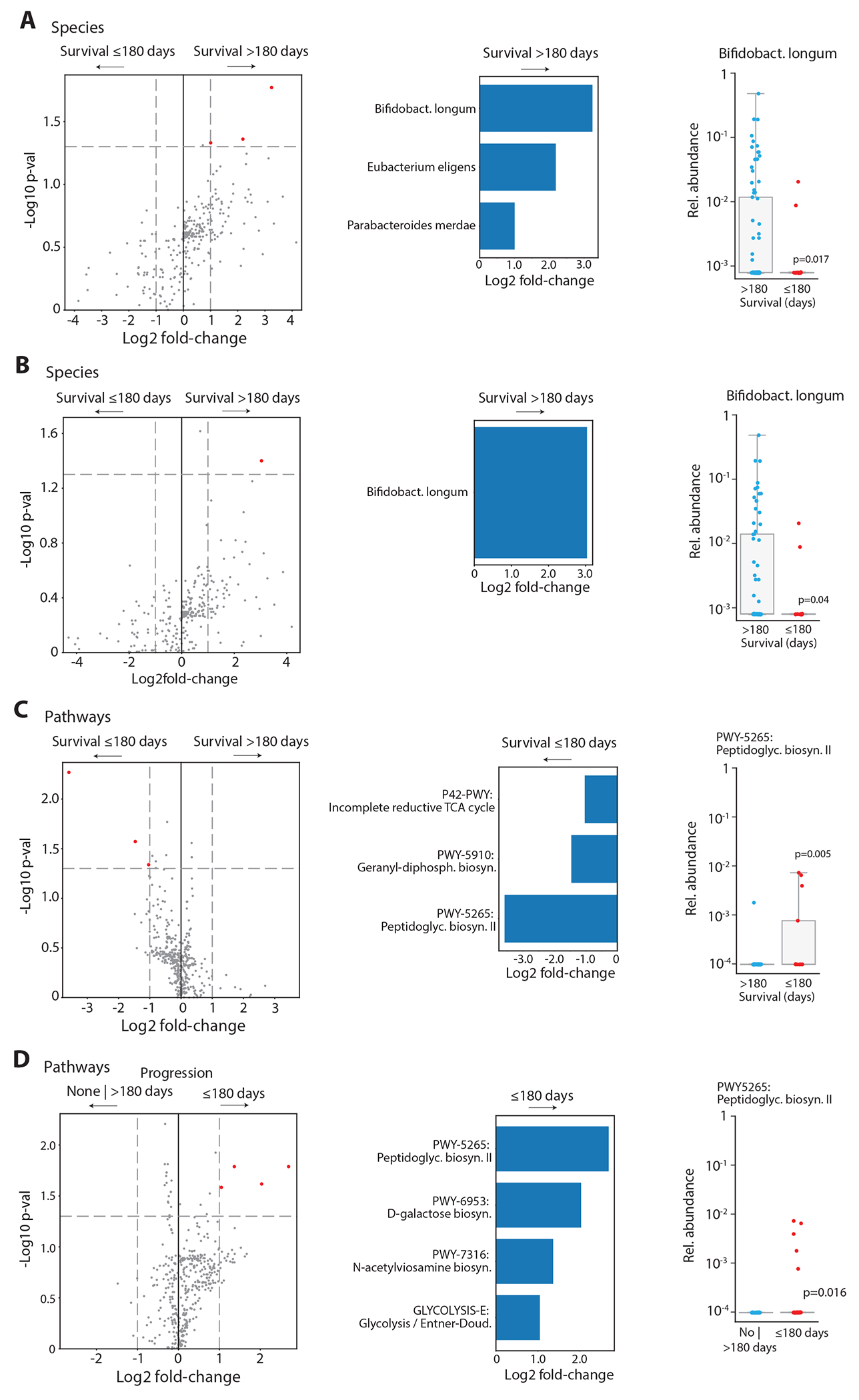
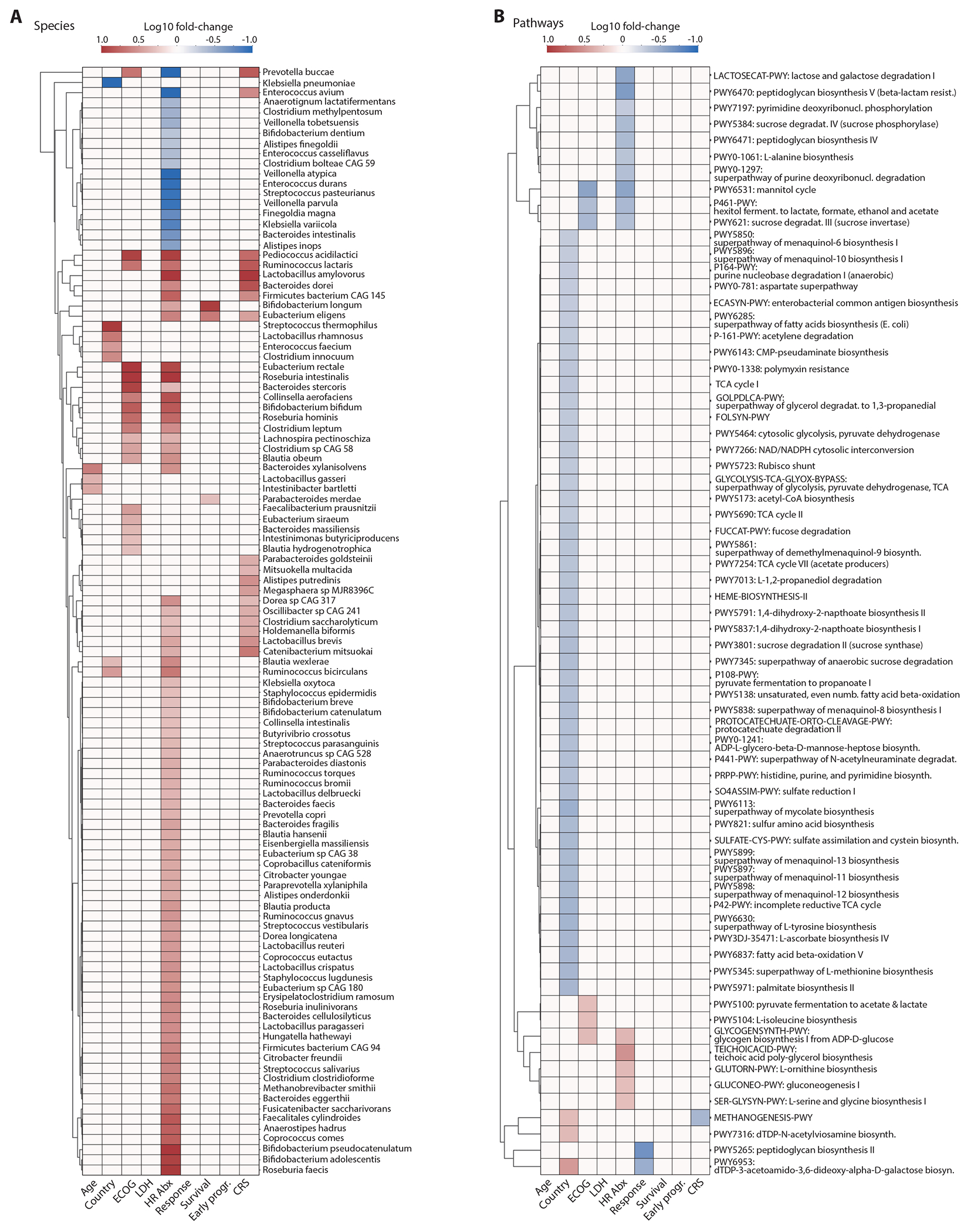
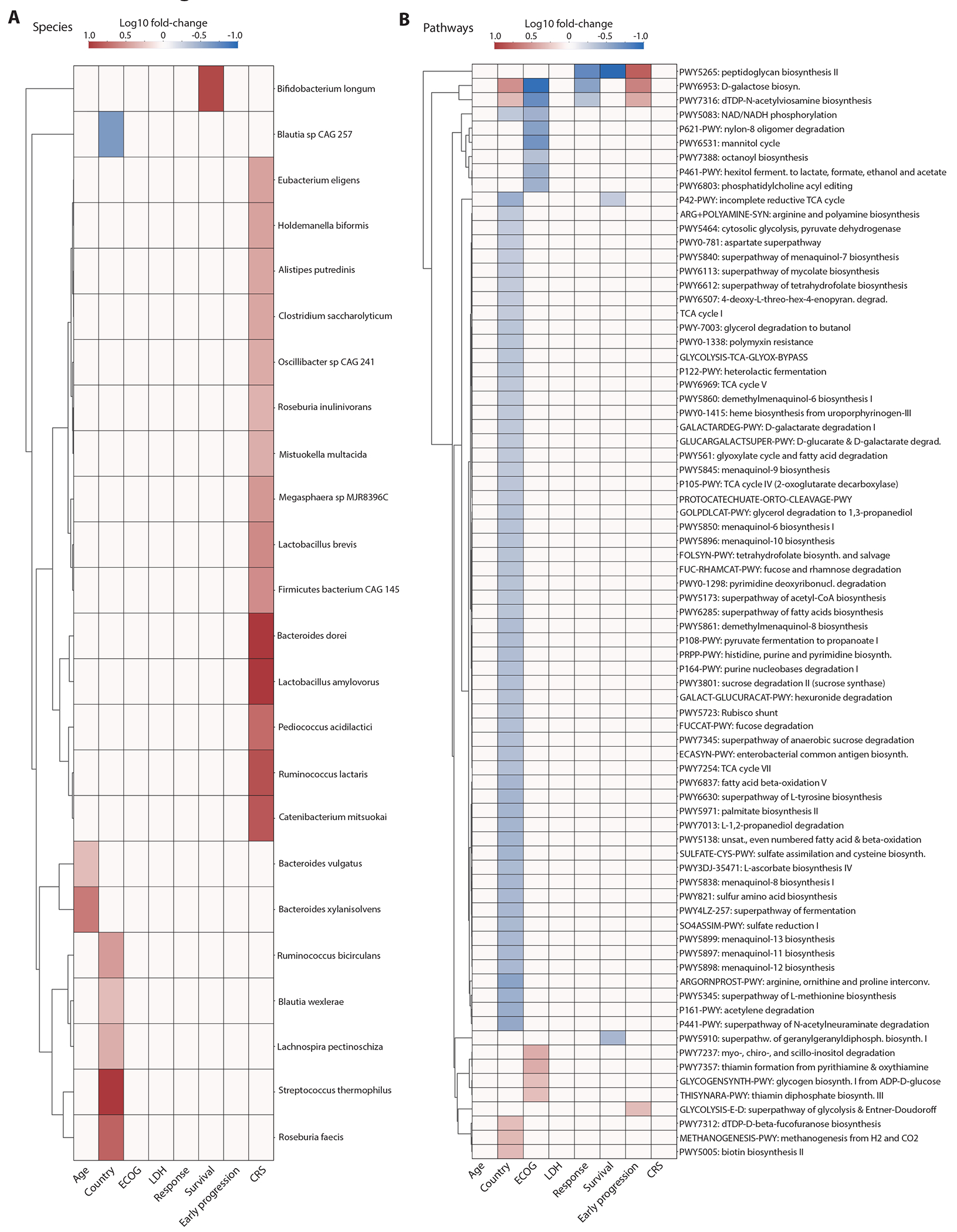
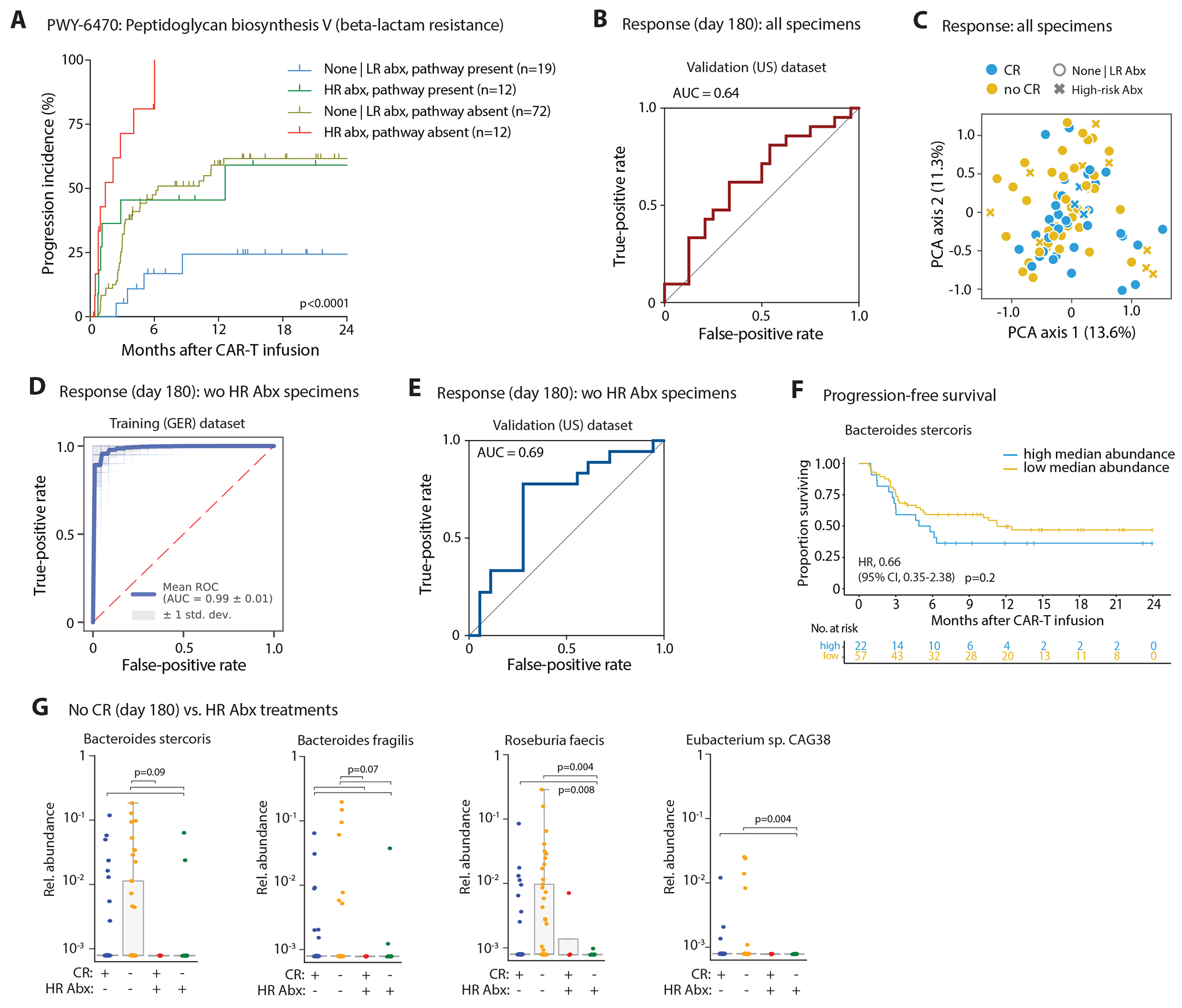
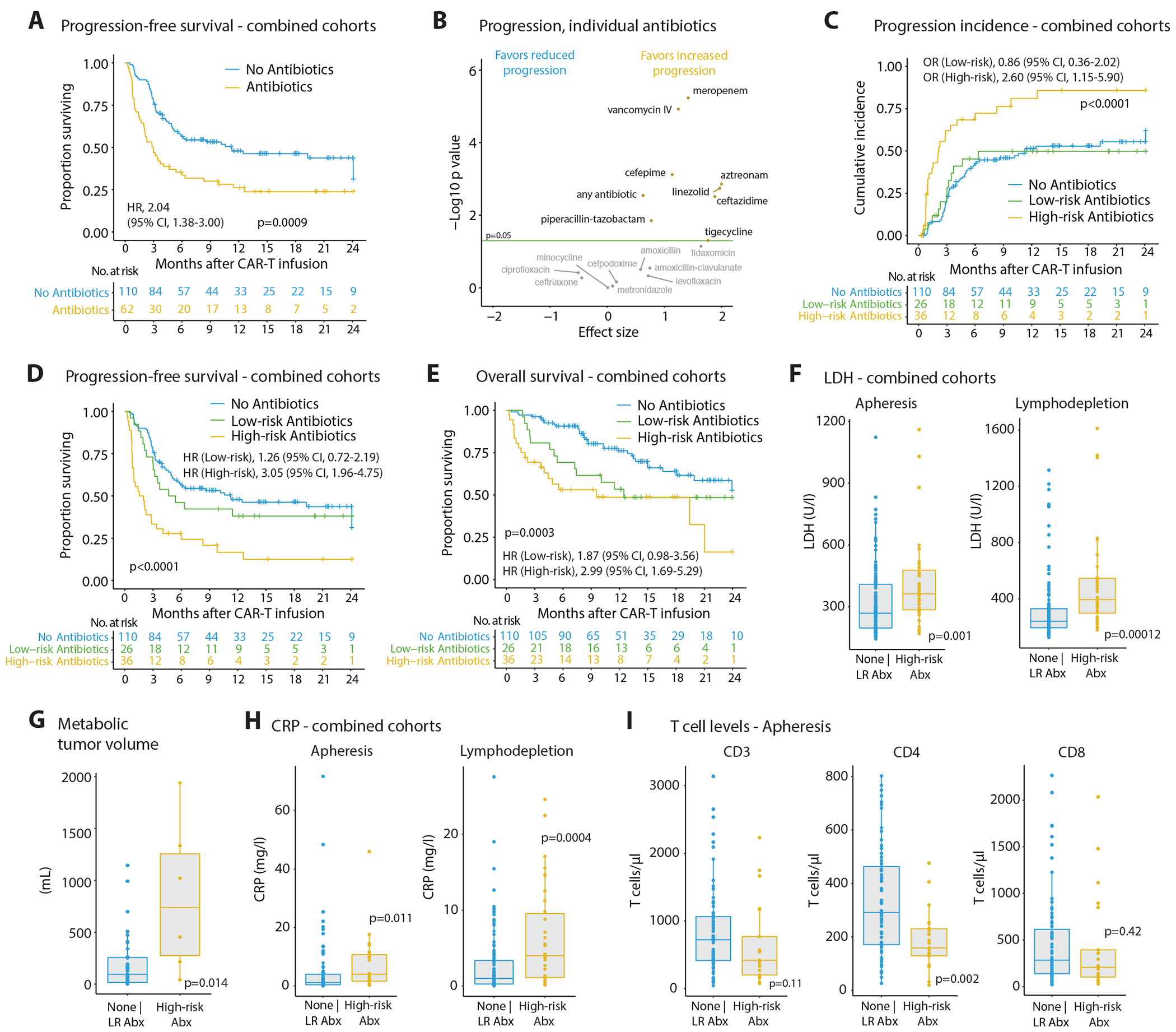
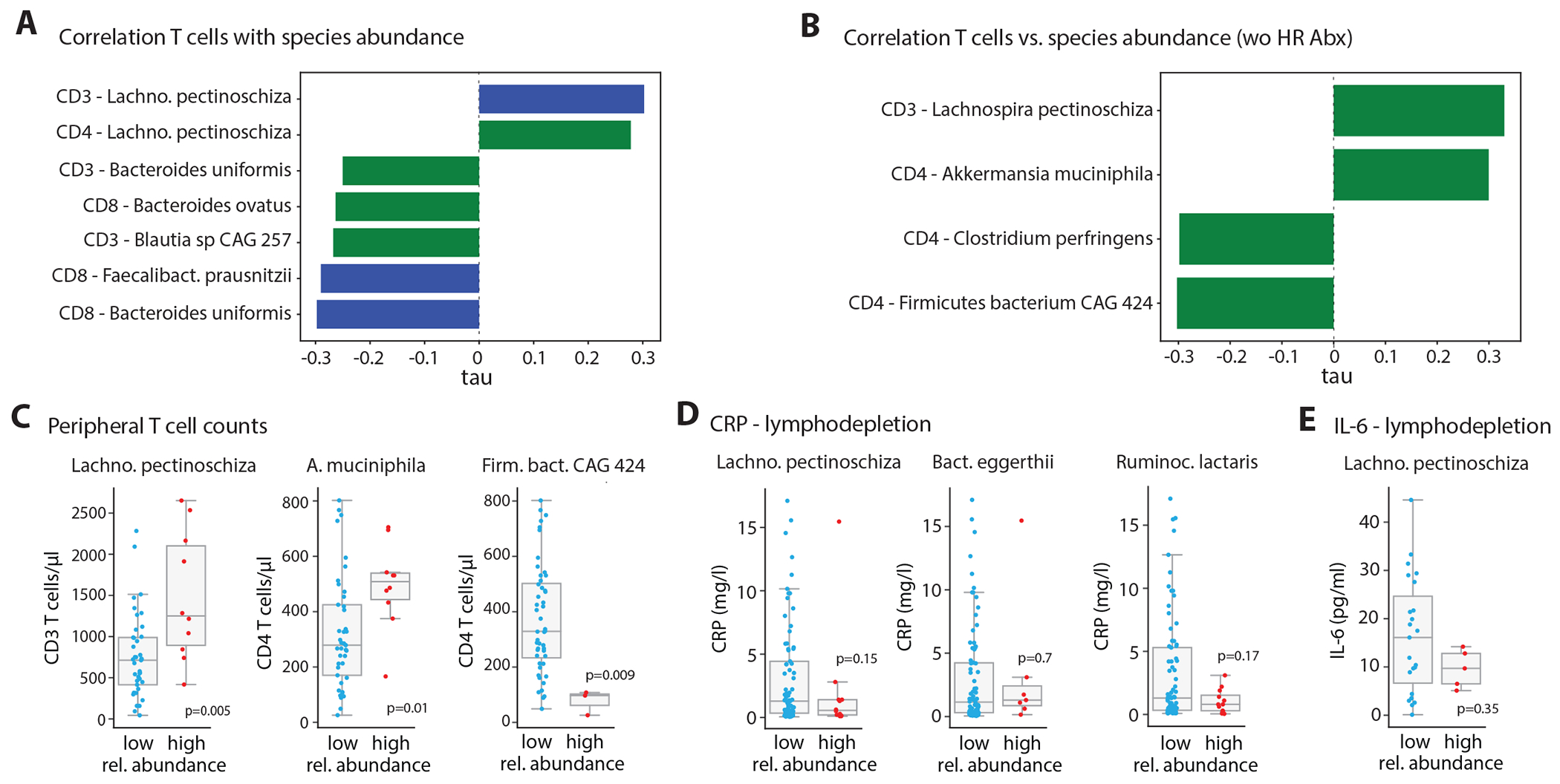
Increasing evidence suggests that the gut microbiome may modulate the efficacy of cancer immunotherapy. In a B cell lymphoma patient cohort from five centers in Germany and the United States (Germany, n = 66; United States, n = 106; total, n = 172), we demonstrate that wide-spectrum antibiotics treatment ('high-risk antibiotics') prior to CD19-targeted chimeric antigen receptor (CAR)-T cell therapy is associated with adverse outcomes, but this effect is likely to be confounded by an increased pretreatment tumor burden and systemic inflammation in patients pretreated with high-risk antibiotics. To resolve this confounding effect and gain insights into antibiotics-masked microbiome signals impacting CAR-T efficacy, we focused on the high-risk antibiotics non-exposed patient population. Indeed, in these patients, significant correlations were noted between pre-CAR-T infusion Bifidobacterium longum and microbiome-encoded peptidoglycan biosynthesis, and CAR-T treatment-associated 6-month survival or lymphoma progression. Furthermore, predictive pre-CAR-T treatment microbiome-based machine learning algorithms trained on the high-risk antibiotics non-exposed German cohort and validated by the respective US cohort robustly segregated long-term responders from non-responders. Bacteroides, Ruminococcus, Eubacterium and Akkermansia were most important in determining CAR-T responsiveness, with Akkermansia also being associated with pre-infusion peripheral T cell levels in these patients. Collectively, we identify conserved microbiome features across clinical and geographical variations, which may enable cross-cohort microbiome-based predictions of outcomes in CAR-T cell immunotherapy.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
V.B. received research funding from Bristol Myers-Sqibb (BMS)/Celgene, Gilead, Janssen, Novartis, Roche and Takeda; V.B. received honoraria from Gilead, Janssen and Novartis. M.-L.S. is a consultant for Novartis, Gilead and Janssen. H.P. is a consultant for Gilead, Abbvie, Pfizer, Novartis, Servier, and BMS. H.P. received research funding from BMS. H.P. received honoraria from Novartis, Gilead, Abbvie, BMS, Servier and Janssen-Cilag. M.L.D. reports consultancy/advisory/honoraria for Kite/Gilead, Novartis, Atara, Precision Biosciences, Celyad, Bellicum, GSK, Adaptive Biotech, and Anixa Biosciences, and research funding from Kite/Gilead, Novartis, and Atara. FLL reports consultancy/advisory for Allogene, Amgen, Bluebird Bio, BMS/Celgene, Calibr, Cellular Biomedicine Group, Cowen, EcoR1, Emerging Therapy Solutions, GammaDelta Therapeutics, Gerson Lehrman Groupt, Iovance, Kite Pharma, Janssen, Legend Biotech, Novartis, Sana, Takeda, Wugen, and Umoja, and research funding from Kite/Gilead, Allogene, Novartis, BlueBird Bio, BMS, NCI, Leukemia and Lymphoma Society, and education or editorial activity for Aptitude Health, ASH, BioPharma Communications CARE Education, Clinical Care Options Oncology, Imedex, Society for Immunotherapy of Cancer. M.D.J. reports consultancy/advisory for Kite/Gilead, Novartis, BMS, MyeloidTx, and research funding from Incyte and Kite/Gilead. The remaining authors declare no competing interests. E.E. is a scientific cofounder of DayTwo and BiomX, and an advisor to Hello Inside, Igen, and Aposense in topics unrelated to this work.
Figures






Comment in
-
Linking the microbiome to CAR-T cell responses.Nat Med. 2023 Apr;29(4):785-786. doi: 10.1038/s41591-023-02272-0. Nat Med. 2023. PMID: 36973411 No abstract available.
References
METHODS-ONLY REFERENCES:
-
- Hastie T TR, Friedman J The Elements of Statistical Learning: Data Mining, Inference, and Prediction. Second edn, 767 (Springer, 2009).
-
- McElreath R A Bayesian Course with Examples in R and STAN. 2nd edn, 612 (Chapman & Hall, 2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
