

Accuracy of sentinel node mapping in patients with biopsy-proven metastatic axillary lymph nodes and upfront surgery: preliminary results of the Multimodal Targeted Axillary Surgery (MUTAS) trial
- PMID: 36915822
- PMCID: PMC10005988
- DOI: 10.21037/gs-22-480
Accuracy of sentinel node mapping in patients with biopsy-proven metastatic axillary lymph nodes and upfront surgery: preliminary results of the Multimodal Targeted Axillary Surgery (MUTAS) trial
Abstract
Background: Some studies suggested that the patients included in the Z0011 trial may represent patients with ultrasound-negative axillary nodes and axillary invasion diagnosed by sentinel node (SN) biopsy. Nevertheless, the National Comprehensive Cancer Network (NCCN) guidelines recommend SN mapping if 1 or 2 suspicious lymph nodes are identified on axillary ultrasound (AU). The aim of this preliminary phase of the Multimodal Targeted Axillary Surgery (MUTAS) trial was to establish the accuracy of SN mapping in patients with axillary involvement undergoing upfront surgery.
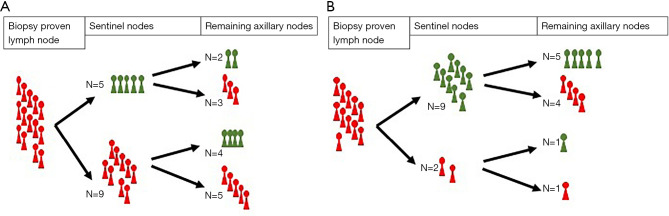
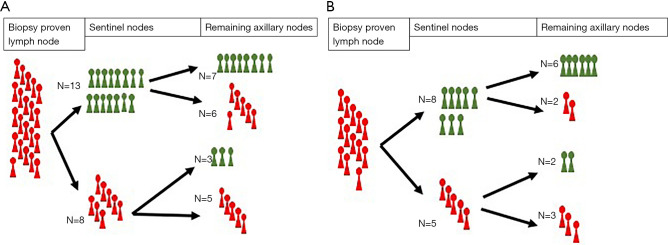
Methods: Between September 2019 and March 2022, we recruited patients with biopsy-proven metastatic axillary nodes and upfront surgery from a single center. We performed SN mapping in these patients before the surgical intervention, which included axillary lymph node dissection. The biopsy-proven metastatic node, SNs and the remaining axillary nodes were excised separately. SN status was considered representative of the status of the remaining axillary nodes. We calculated the sensitivity, specificity, negative predictive value and positive predictive value of the SN, overall and in patients with palpable nodes, in those with non-palpable nodes and an AU leading to diagnosis of axillary involvement, in those with 1 or 2 suspicious nodes on AU, and in patients with a single suspicious node on AU. We evaluated clinical, imaging and pathology features as predictors of the status of the remaining axillary nodes, false-negatives, and false-positives.
Results: We included 25 patients in this phase. The false-negative rate of SN mapping was 28% overall, 21.42% for patients with palpable nodes, 36.36% for patients with non-palpable nodes and an AU diagnosis of axillary involvement, 28.75% for those with 1 or 2 suspicious nodes on AU, and 15.38% in patients with a single suspicious node on AU. The negative predictive value was highest in patients with a single suspicious node on AU (75%). The only significant predictive factor was that FN showed a higher Ki67 index score.
Conclusions: In this study, SN mapping was not reliable in patients with biopsy-proven metastatic axillary nodes and upfront surgery for any of the subgroups studied. Further research should elucidate the best staging pathways in these patients to avoid premature de-escalation.
Keywords: Breast cancer; biopsy-proven lymph nodes; false-negatives; non-palpable lymph nodes; sentinel nodes (SNs).
2023 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://gs.amegroups.com/article/view/10.21037/gs-22-480/coif). The authors have no conflicts of interest to declare.
Figures
Comment in
-
Axillary surgery in the case of limited involved axillary lymph nodes.Gland Surg. 2023 Jun 30;12(6):727-729. doi: 10.21037/gs-23-109. Epub 2023 May 25. Gland Surg. 2023. PMID: 37441013 Free PMC article. No abstract available.
-
Can targeted axillary dissection reliably advise de-escalation of completion axillary lymph node dissection?Gland Surg. 2023 Jun 30;12(6):730-732. doi: 10.21037/gs-23-106. Epub 2023 May 22. Gland Surg. 2023. PMID: 37441015 Free PMC article. No abstract available.
References
-
- Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol 2010;11:927-33. 10.1016/S1470-2045(10)70207-2 - DOI - PMC - PubMed
-
- Giuliano AE, Ballman KV, McCall L, et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017;318:918-26. 10.1001/jama.2017.11470 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous