

Upper gastrointestinal bleeding in adults treated with veno-arterial extracorporeal membrane oxygenation: a cohort study
- PMID: 36916745
- PMCID: PMC10089675
- DOI: 10.1093/ejcts/ezad083
Upper gastrointestinal bleeding in adults treated with veno-arterial extracorporeal membrane oxygenation: a cohort study
Abstract
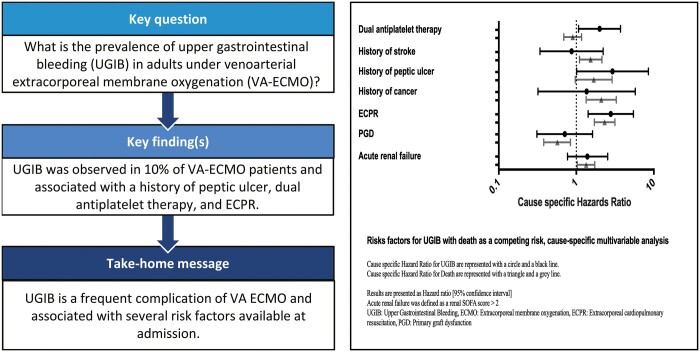
Objectives: Upper gastrointestinal bleeding (UGIB) is a common complication in adults treated with veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for refractory cardiogenic shock or cardiac arrest. We aimed to determine risk factors, prevalence and outcomes associated with VA-ECMO-associated UGIB in adult patients.
Methods: We conducted a retrospective cohort study (2014-2022) on consecutive VA-ECMO patients in the medical and infectious disease intensive care unit of Bichat-Claude Bernard University Hospital, Paris, France. UGIB was defined as (i) an overt bleeding (haematemesis, melena, haematochezia) or (ii) acute anaemia associated with a lesion diagnosed on upper gastrointestinal endoscopy. VA-ECMO-associated UGIB was defined as an UGIB occurring during VA-ECMO, or up to 10 days after decannulation in patients weaned off extracorporeal membrane oxygenation (ECMO). Cause-specific models were used to identify factors associated with UGIB and death, respectively.
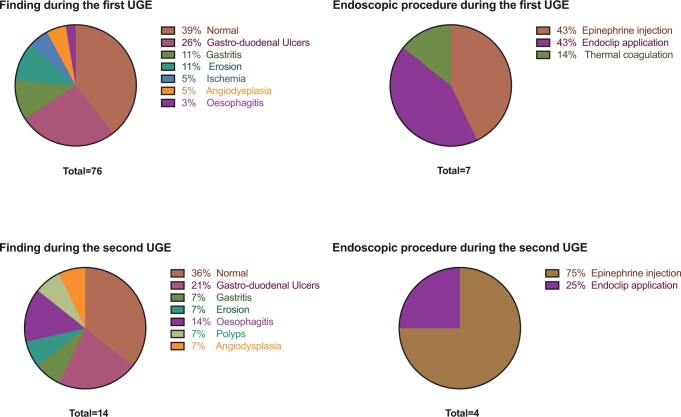
Results: Among the 455 patients included, 48 (10%) were diagnosed with UGIB after a median of 12 [7; 23] days following ECMO cannulation. Mortality occurred in 36 (75%) patients with UGIB and 243 (60%) patients without. UGIB patients had longer intensive care unit stays (32 [19; 60] vs 18 [7; 37] days; P < 0.01), longer ECMO (14 [9; 18] vs 7 [4; 11] days; P < 0.01) and mechanical ventilation durations (21 [16; 36] vs 10 [5; 20] days; P < 0.01), as compared to non-UGIB patients. Ninety upper gastrointestinal endoscopies were performed, and the most frequent lesions detected were gastro-duodenal ulcers (n = 23, 26%), leading to 11/90 therapeutic procedures. By multivariable analysis, a history of peptic ulcer [cause-specific hazard ratio (CSHR) 2.93, 95% confidence interval (CI) [1.01; 8.51]], a dual antiplatelet therapy (CSHR 2.0, 95% CI [1.07; 3.72]) and extracorporeal cardiopulmonary resuscitation (CSHR 2.78, 95% CI [1.42; 5.45]) were independently associated with an increased risk of UGIB.
Conclusions: In adult patients under VA-ECMO, a history of gastric ulcer, dual antiplatelet therapy and extracorporeal cardiopulmonary resuscitation were independently associated with an increased risk of UGIB. This study highlights the potential role of acute ischaemia-reperfusion injury in the pathophysiology of VA-ECMO-associated UGIB.
Keywords: Endoscopy; Extracorporeal membrane oxygenation; Gastrointestinal haemorrhage; Intensive care units; Shock; cardiogenic; gastrointestinal.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Comment in
-
Upper gastrointestinal bleeding in veno-arterial extracorporeal membrane oxygenation patients: a neglected (sometimes hidden) enemy deserving further investigation and action.Eur J Cardiothorac Surg. 2023 Apr 3;63(4):ezad148. doi: 10.1093/ejcts/ezad148. Eur J Cardiothorac Surg. 2023. PMID: 37079722 No abstract available.
References
-
- Karagiannidis C, Brodie D, Strassmann S, Stoelben E, Philipp A, Bein T. et al. Extracorporeal membrane oxygenation: evolving epidemiology and mortality. Intensive Care Med 2016;42:889–96. - PubMed
-
- Mao J, Paul S, Sedrakyan A.. The evolving use of ECMO: the impact of the CESAR trial. Int J Surg 2016;35:95–9. - PubMed
-
- Liolios A, Oropello JM, Benjamin E.. Gastrointestinal complications in the intensive care unit. Clin Chest Med 1999;20:329–45, viii. - PubMed
