

Expanding the Phenotypic Spectrum of Kenny-Caffey Syndrome
- PMID: 36916904
- PMCID: PMC10438882
- DOI: 10.1210/clinem/dgad147
Expanding the Phenotypic Spectrum of Kenny-Caffey Syndrome
Abstract
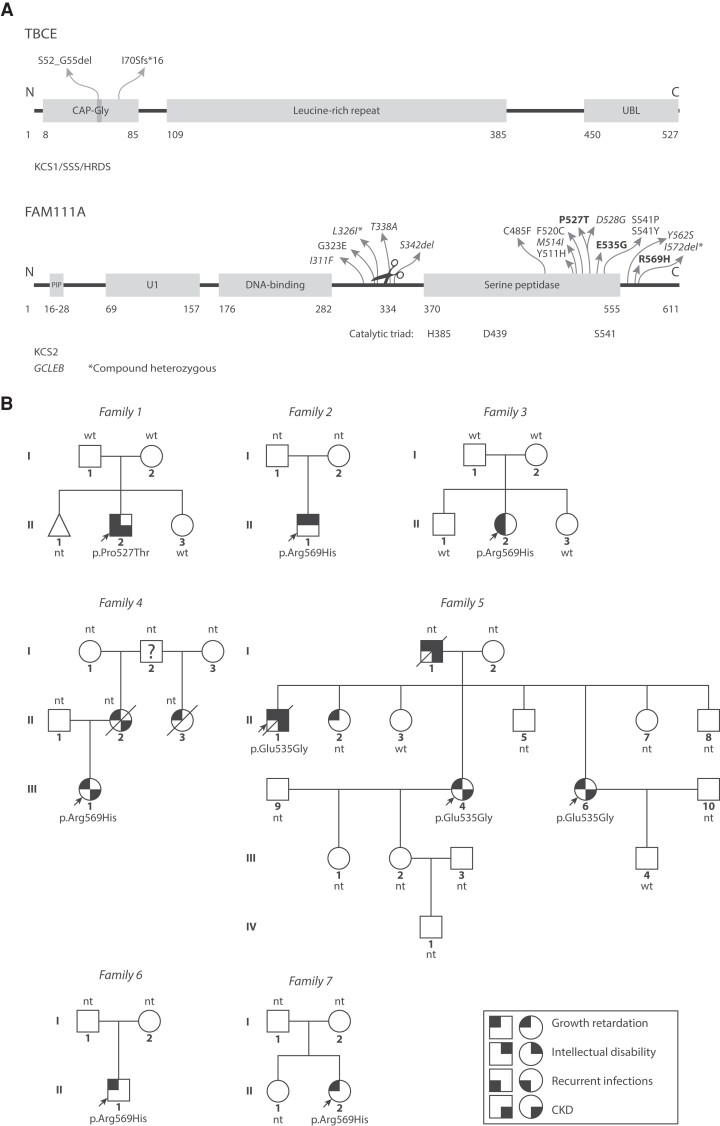
Context: Kenny-Caffey syndrome (KCS) is a rare hereditary disorder characterized by short stature, hypoparathyroidism, and electrolyte disturbances. KCS1 and KCS2 are caused by pathogenic variants in TBCE and FAM111A, respectively. Clinically the phenotypes are difficult to distinguish.
Objective: The objective was to determine and expand the phenotypic spectrum of KCS1 and KCS2 in order to anticipate complications that may arise in these disorders.
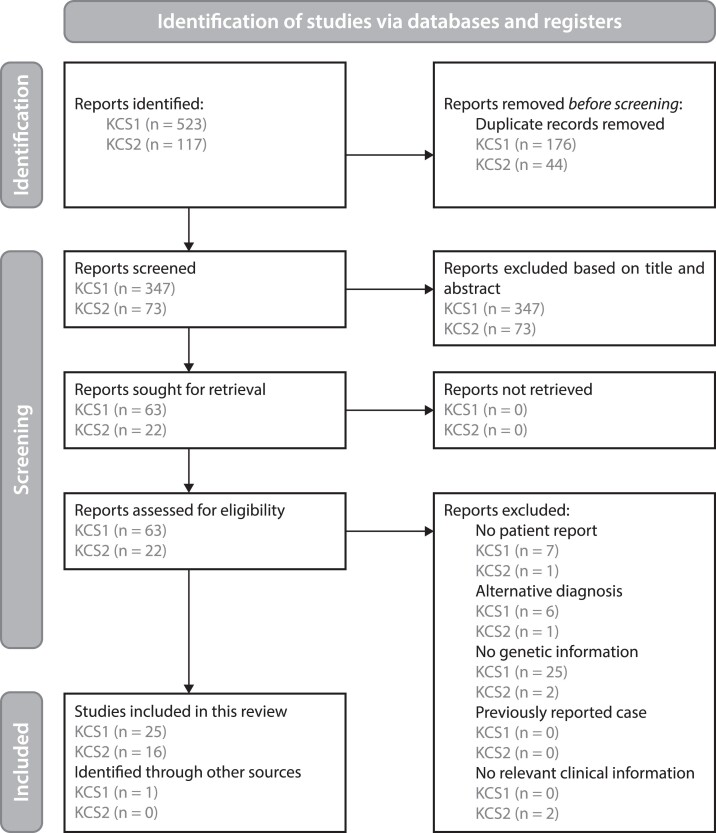
Methods: We clinically and genetically analyzed 10 KCS2 patients from 7 families. Because we found unusual phenotypes in our cohort, we performed a systematic review of genetically confirmed KCS cases using PubMed and Scopus. Evaluation by 3 researchers led to the inclusion of 26 papers for KCS1 and 16 for KCS2, totaling 205 patients. Data were extracted following the Cochrane guidelines and assessed by 2 independent researchers.
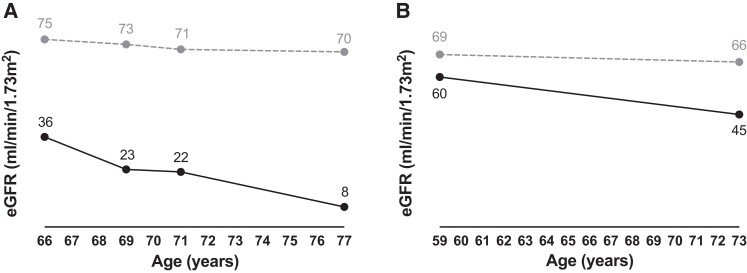
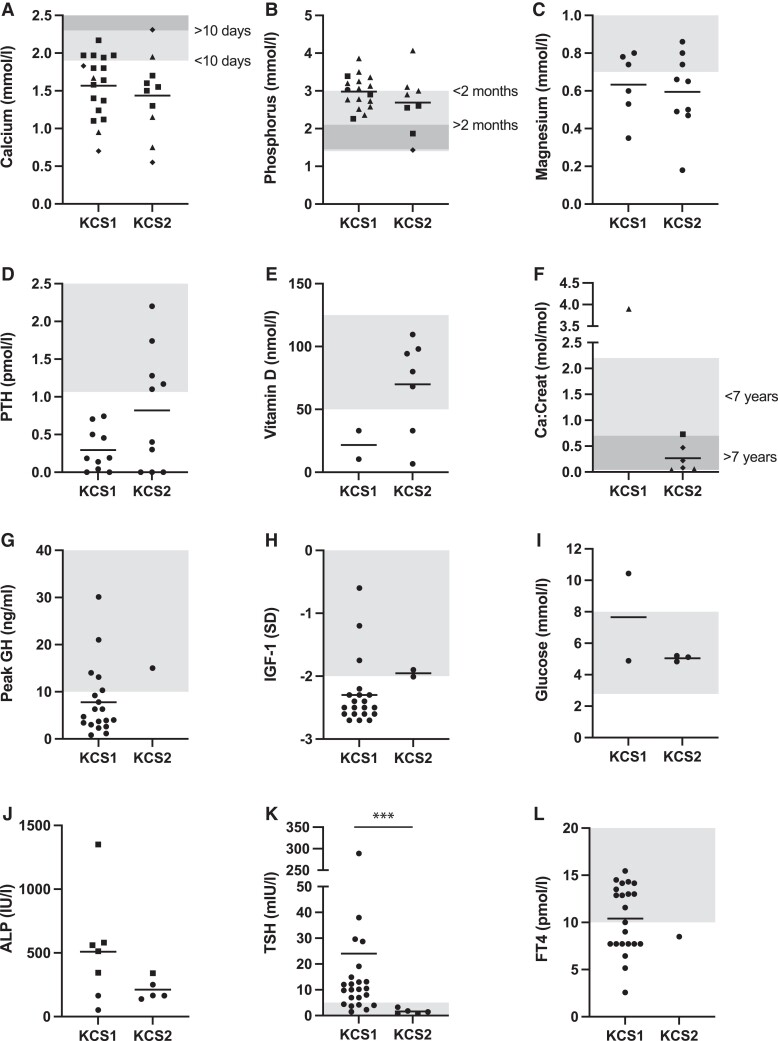
Results: Several patients in our KCS2 cohort presented with intellectual disability (3/10) and chronic kidney disease (6/10), which are not considered common findings in KCS2. Systematic review of all reported KCS cases showed that the phenotypes of KCS1 and KCS2 overlap for postnatal growth retardation (KCS1: 52/52, KCS2: 23/23), low parathyroid hormone levels (121/121, 16/20), electrolyte disturbances (139/139, 24/27), dental abnormalities (47/50, 15/16), ocular abnormalities (57/60, 22/23), and seizures/spasms (103/115, 13/16). Symptoms more prevalent in KCS1 included intellectual disability (74/80, 5/24), whereas in KCS2 bone cortical thickening (1/18, 16/20) and medullary stenosis (7/46, 27/28) were more common.
Conclusion: Our case series established chronic kidney disease as a new feature of KCS2. In the literature, we found substantial overlap in the phenotypic spectra of KCS1 and KCS2, but identified intellectual disability and the abnormal bone phenotype as the most distinguishing features.
Keywords: Sanjad–Sakati syndrome; chronic kidney disease; gracile bone dysplasia; hypoparathyroidism retardation dysmorphism; osteocraniostenosis.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Kenny FM, Linarelli L. Dwarfism and cortical thickening of tubular bones. Transient hypocalcemia in a mother and son. Am J Dis Child. 1966;111(2):201‐207. - PubMed
-
- Caffey J. Congenital stenosis of medullary spaces in tubular bones and calvaria in two proportionate dwarfs—mother and son; coupled with transitory hypocalcemic tetany. Am J Roentgenol Radium Ther Nucl Med. 1967;100(1):1‐11. - PubMed
-
- Parvari R, Hershkovitz E, Grossman N, et al. Mutation of TBCE causes hypoparathyroidism-retardation-dysmorphism and autosomal recessive Kenny-Caffey syndrome. Nat Genet. 2002;32(3):448‐452. - PubMed
-
- Serna M, Carranza G, Martín-Benito J, et al. The structure of the complex between α-tubulin, TBCE and TBCB reveals a tubulin dimer dissociation mechanism. J Cell Sci. 2015;128(9):1824‐1834. - PubMed
