

Medicare Advantage Enrollment Among Beneficiaries With End-Stage Renal Disease in the First Year of the 21st Century Cures Act
- PMID: 36917063
- PMCID: PMC10015314
- DOI: 10.1001/jama.2023.1426
Medicare Advantage Enrollment Among Beneficiaries With End-Stage Renal Disease in the First Year of the 21st Century Cures Act
Abstract
Importance: Before 2021, most Medicare beneficiaries with end-stage renal disease (ESRD) were unable to enroll in private Medicare Advantage (MA) plans. The 21st Century Cures Act permitted these beneficiaries to enroll in MA plans effective January 2021.
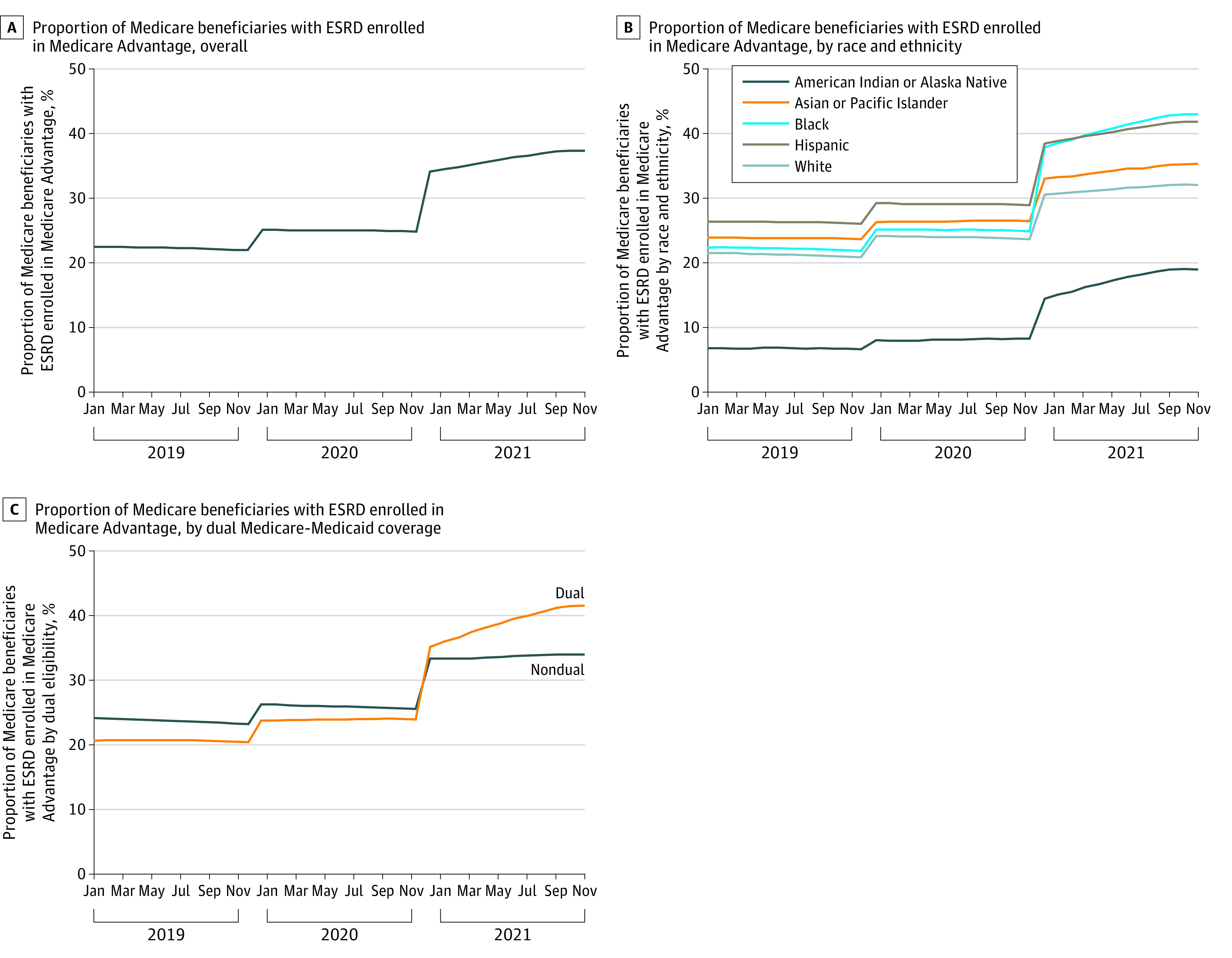
Objective: To examine changes in MA enrollment among Medicare beneficiaries with ESRD after enactment of the 21st Century Cures Act overall and by race or ethnicity and dual-eligible status.
Design, setting, and participants: This cross-sectional time-trend study used data from Medicare beneficiaries with ESRD (both kidney transplant recipients and those undergoing dialysis) between January 2019 and December 2021. Data were analyzed between June and October 2022.
Exposures: 21st Century Cures Act.
Main outcomes and measures: Primary outcomes were the proportion of Medicare beneficiaries with prevalent ESRD who switched from traditional Medicare to MA between 2020 and 2021 and those with incident ESRD who newly enrolled in MA in 2021. Individuals who stayed in traditional Medicare were enrolled in 2020 and 2021 and those who switched to MA were enrolled in traditional Medicare in 2020 and MA in 2021.
Results: Among 575 797 beneficiaries with ESRD in 2020 or 2021 (mean [SD] age, 64.7 [14.2] years, 42.2% female, 34.0% Black, and 7.7% Hispanic or Latino), the proportion of beneficiaries enrolled in MA increased from 24.8% (December 2020) to 37.4% (December 2021), a relative change of 50.8%. The largest relative increases in MA enrollment were among Black (72.8% relative increase), Hispanic (44.8%), and dual-eligible beneficiaries with ESRD (73.6%). Among 359 617 beneficiaries with TM and prevalent ESRD in 2020, 17.6% switched to MA in 2021. Compared with individuals who stayed in traditional Medicare, those who switched to MA had modestly more chronic conditions (6.3 vs 6.1; difference, 0.12 conditions [95% CI, 0.10-0.16]) and similar nondrug spending in 2020 (difference, $509 [95% CI, -$58 to $1075]) but were more likely to be Black (difference, 19.5 percentage points [95% CI, 19.1-19.9]) and have dual Medicare-Medicaid eligibility (difference, 20.8 percentage points [95% CI, 20.4-21.2]). Among beneficiaries who were newly eligible for Medicare ESRD benefits in 2021, 35.2% enrolled in MA.
Conclusions and relevance: Results suggest that increases in MA enrollment among Medicare beneficiaries with ESRD were substantial the first year after the 21st Century Cures Act, particularly among Black, Hispanic, and dual-eligible individuals. Policy makers and MA plans may need to assess network adequacy, disenrollment, and equity of care for beneficiaries who enrolled in MA.
Conflict of interest statement
Figures
Comment on
-
Early Findings From Medicare's End-Stage Renal Disease Treatment Choices Model.JAMA Health Forum. 2022 Oct 7;3(10):e223500. doi: 10.1001/jamahealthforum.2022.3500. JAMA Health Forum. 2022. PMID: 36206008 Free PMC article. No abstract available.
References
-
- US Renal Data System. 2020 USRDS annual data report: epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2021. Accessed February 16, 2023. https://adr.usrds.org/2020
-
- 21st Century Cures Act, HR 34, 114th Cong (2015).
-
- Federal Register. Medicare and Medicaid programs: contract year 2021 and 2022 policy and technical changes to the Medicare Advantage program, Medicare Prescription Drug Benefit program, Medicaid program, Medicare Cost Plan program, and programs of all-inclusive care for the elderly. Proposed rule. February 18, 2020. Accessed February 16, 2023. https://www.federalregister.gov/documents/2020/02/18/2020-02085/medicare...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
