

Leveraging a nationwide infection surveillance program to implement a colorectal surgical site infection reduction bundle: a pragmatic, prospective, and multicenter cohort study
- PMID: 36917127
- PMCID: PMC10389383
- DOI: 10.1097/JS9.0000000000000277
Leveraging a nationwide infection surveillance program to implement a colorectal surgical site infection reduction bundle: a pragmatic, prospective, and multicenter cohort study
Abstract
Background: Bundled interventions usually reduce surgical site infection (SSI) when implemented at single hospitals, but the feasibility of their implementation at the nationwide level and their clinical results are not well established.
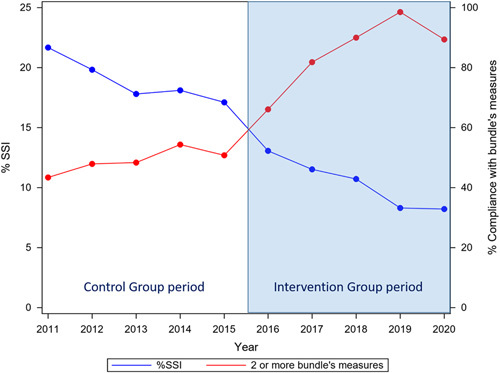
Materials and methods: Pragmatic interventional study to analyze the implementation and outcomes of a colorectal surgery care bundle within a nationwide quality improvement program. The bundle consisted of antibiotic prophylaxis, oral antibiotic prophylaxis (OAP), mechanical bowel preparation, laparoscopy, normothermia, and a wound retractor. Control group (CG) and Intervention group (IG) were compared. Overall SSI, superficial (S-SSI), deep (D-SSI), and organ/space (O/S-SSI) rates were analyzed. Secondary endpoints included microbiology, 30-day mortality, and length of hospital stay.
Results: A total of 37 849 procedures were included, 19 655 in the CG and 18 194 in the IG. In all, 5462 SSIs (14.43%) were detected: 1767 S-SSI (4.67%), 847 D-SSI (2.24%), and 2838 O/S-SSI (7.5%). Overall SSI fell from 18.38% (CG) to 10.17% (IG), odds ratio (OR) of 0.503 [0.473-0.524]. O/S-SSI rates were 9.15% (CG) and 5.72% (IG), OR of 0.602 [0.556-0.652]. The overall SSI rate was 16.71% when no measure was applied and 6.23% when all six were used. Bundle implementation reduced the probability of overall SSI (OR: 0.331; CI 95 : 0.242-0.453), and also O/S-SSI rate (OR: 0.643; CI 95 : 0.416-0.919). In the univariate analysis, all measures except normothermia were associated with a reduction in overall SSI, while only laparoscopy, OAP, and mechanical bowel preparation were related to a decrease in O/S-SSI. Laparoscopy, wound retractor, and OAP decreased overall SSI and O/S-SSI in the multivariate analysis.
Conclusions: In this cohort study, the application of a specific care bundle within a nationwide nosocomial infection surveillance system proved feasible and resulted in a significant reduction in overall and O/S-SSI rates in the elective colon and rectal surgery. The OR for SSI fell between 1.5 and 3 times after the implementation of the bundle.
Trial registration: ClinicalTrials.gov NCT04129177.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflict of interest. All authors submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures







References
-
- ECDC, European Centre for Disease Prevention and Control. Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals 2011.2012; 2013. Accessed 20 May 2022. https://ecdc.europa.eu/sites/portal/file
-
- Keenan JE, Speicher PJ, Thacker JKM, et al. The preventive surgical site infection bundle in colorectal surgery an effective approach to surgical site infection reduction and health care cost savings. JAMA Surg 2014;149:1045–52. - PubMed
-
- Pastor C, Baek JH, Varma MG, et al. Validation of the risk index category as a predictor of surgical site infection in elective colorectal surgery. Dis Colon Rectum 2010;53:721–727. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
