

Hospitalization Rates for Inflammatory Bowel Disease Are Decreasing Over Time: A Population-based Cohort Study
- PMID: 36917200
- PMCID: PMC10547231
- DOI: 10.1093/ibd/izad020
Hospitalization Rates for Inflammatory Bowel Disease Are Decreasing Over Time: A Population-based Cohort Study
Abstract
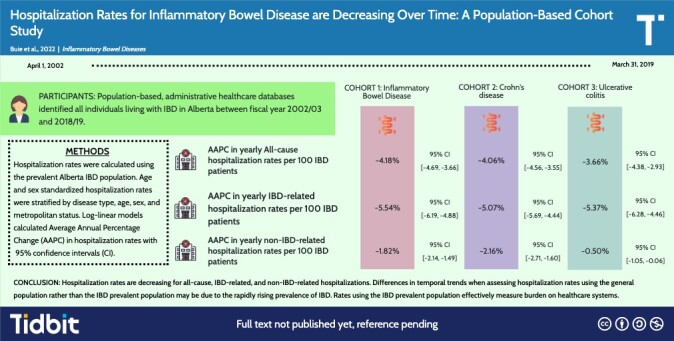
Background: Recent advances in the management of inflammatory bowel disease (IBD) striving for new treatment targets may have decreased rates of hospitalization for flares. We compared all-cause, IBD-related, and non-IBD-related hospitalizations while accounting for the rising prevalence of IBD.
Methods: Population-based, administrative health care databases identified all individuals living with IBD in Alberta between fiscal year 2002 and 2018. Hospitalization rates (all-cause, IBD-related, and non-IBD-related) were calculated using the prevalent Alberta IBD population. Hospitalizations were stratified by disease type, age, sex, and metropolitan status. Data were age and sex standardized to the 2019 Canadian population. Log-linear models calculated Average Annual Percentage Change (AAPC) in hospitalization rates with associated 95% confidence intervals (CIs).
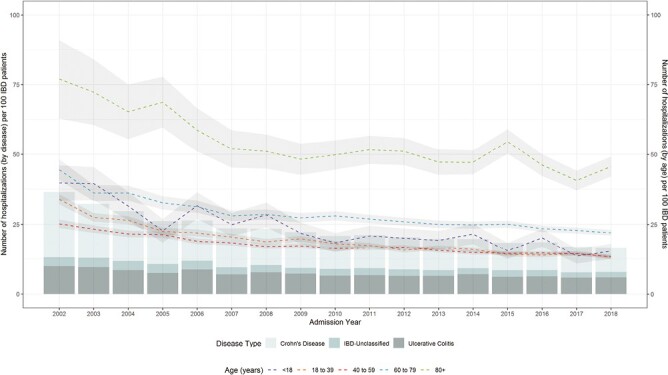
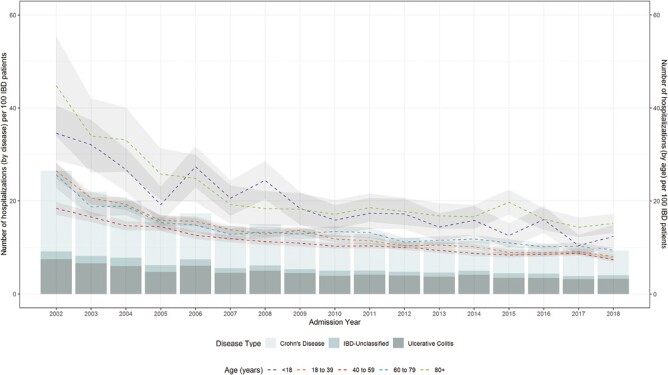
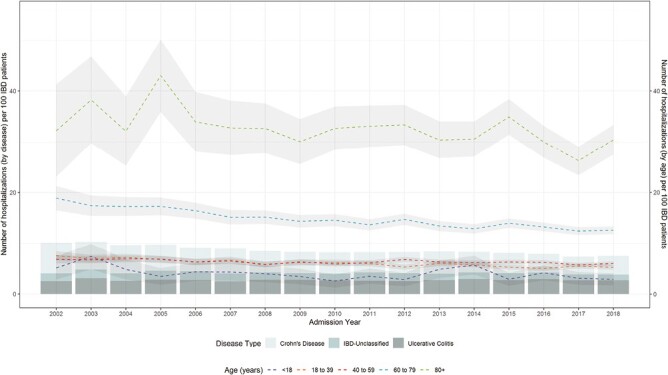
Results: From 2002-2003 to 2018-2019, all-cause hospitalization rates decreased from 36.57 to 16.72 per 100 IBD patients (AAPC, -4.18%; 95% CI, -4.69 to -3.66). Inflammatory bowel disease-related hospitalization rate decreased from 26.44 to 9.24 per 100 IBD patients (AAPC, -5.54%; 95% CI, -6.19 to -4.88). Non-IBD-related hospitalization rate decreased from 10.13 to 7.48 per 100 IBD patients (AAPC, -1.82%; 95% CI, -2.14 to -1.49). Those over 80 years old had the greatest all-cause and non-IBD-related hospitalization rates. Temporal trends showing decreasing hospitalization rates were observed across age, sex, IBD type, and metropolitan status.
Conclusions: Hospitalization rates are decreasing for all-cause, IBD-related, and non-IBD-related hospitalizations. Over the past 20 years, the care of IBD has transitioned from hospital-based care to ambulatory-centric IBD management.
Keywords: Crohn’s disease; epidemiology; hospitalization rates; inflammatory bowel disease; ulcerative colitis.
Plain language summary
Hospitalization rates per 100 IBD patients are decreasing. However, when using the general population as the denominator, the interpretation of temporal trends changes because the prevalence of IBD has risen faster than the general population’s growth rate.
© 2023 Crohn’s & Colitis Foundation. Published by Oxford University Press on behalf of Crohn’s & Colitis Foundation.
Conflict of interest statement
G.K. has received honoraria for speaking or consultancy from AbbVie, Janssen, Pfizer, Amgen, and Takeda. He has received research support from Ferring, Janssen, AbbVie, GlaxoSmith Kline, Merck, and Shire. He has been a consultant for Gilead. He shares ownership of a patent: TREATMENT OF INFLAMMATORY DISORDERS, AUTOIMMUNE DISEASE, AND PBC. UTI Limited Partnership, assignee. Patent WO2019046959A1. PCT/CA2018/051098. September 7, 2018.
A-A.S. has research grants (investigator initiated programs) from Gilead and Intercept Pharmaceuticals.
H.S. has been on advisory boards or consulted to Pendopharm, Amgen Canada, Bristol Myers Squibb Canada, Roche Canada, Sandoz Canada, Takeda Canada, and Guardant Health, Inc.,
C.B. has consulted to or served on advisory boards for Abbvie Canada, Amgen Canada, Bristol Myers Squibb Canada, JAMP Pharmaceuticals, Janssen Canada, Pfizer Canada, Sandoz Canada, Takeda, and has received unrestricted educational grants from Abbvie Canada, Janssen Canada, Pfizer Canada, Bristol Myers Squibb Canada, and Takeda Canada. He has been on the speaker’s bureau of Abbvie Canada, Janssen Canada, Pfizer Canada, and Takeda Canada. He has received research grants from Abbvie Canada, Amgen Canada, Pfizer Canada, and Sandoz Canada and contract grants from Janssen.
R.P. has received consulting fees from Abbott, AbbVie, Alimentiv (formerly Robarts), Amgen, Arena Pharmaceuticals, AstraZeneca, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Cosmos Pharmaceuticals, Eisai, Elan, Eli Lilly, Ferring, Galapagos, Fresenius Kabi, Genentech, Gilead Sciences, Glaxo-Smith Kline, JAMP Bio, Janssen, Merck, Mylan, Novartis, Oppilan Pharma, Organon, Pandion Pharma, Pendopharm, Pfizer, Progenity, Protagonist Therapeutics, Roche, Sandoz, Satisfai Health, Shire, Sublimity Therapeutics, Takeda.
E.B. has acted as a legal consultant for Hoffman La-Roche Limited and Peabody & Arnold LLP.
A.O. has been on advisory boards of AbbVie Canada, Janssen Canada, and Nestle. He has received unrestricted educational grants from AbbVie Canada and Janssen Canada. His site is involved with clinical trials for AbbVie, Pfizer, Takeda, Eli Lily, and Celgene.
L.T. has received investigator initiated funding from Janssen Canada and served on advisory boards for AbbVie Canada, Sandoz Canada, Takeda Canada, Merck Canada, Pfizer Canada, Janssen Canada, and Roche Canada.
C.M. has received consulting fees from AbbVie, Alimentiv, Amgen, AVIR Pharma Inc, BioJAMP, Bristol Myers Squibb, Celltrion, Ferring, Fresenius Kabi, Janssen, McKesson, Mylan, Takeda, Pendopharm, Pfizer, Roche; speaker’s fees from AbbVie, Amgen, AVIR Pharma Inc, Alimentiv, Bristol Myers Squibb, Ferring, Fresenius Kabi, Janssen, Takeda, Pendopharm, and Pfizer; royalties from Springer Publishing; research support from Ferring, Pfizer.
A.B. has been a member of advisory boards for Abbvie, Pfizer, Takeda, Janssen, Merck and speaker’s bureau for Abbvie, Janssen, Takeda, Pfizer.
J.J. reports advisory board fees from AbbVie, Janssen, Pfizer, Ferring; speaker’s fees from AbbVie, Janssen Takeda; and research support from AbbVie, Janssen and Pfizer.
The following authors have no conflicts to declare: M.B., S.C., S.M., J. P., L.H., E.K., A.A-Z, and J.H-L.
Figures
References
-
- Mao EJ, Hazlewood GS, Kaplan GG, Peyrin-Biroulet L, Ananthakrishnan AN.. Systematic review with meta-analysis: comparative efficacy of immunosuppressants and biologics for reducing hospitalisation and surgery in Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther. Jan 2017;45(1):3-13. doi: 10.1111/apt.13847 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
