

Impacted bone allograft personalised by a novel 3D printed customization kit produces high surgical accuracy in medial opening wedge high tibial osteotomy: a pilot study
- PMID: 36917322
- PMCID: PMC10012299
- DOI: 10.1186/s40634-023-00593-0
Impacted bone allograft personalised by a novel 3D printed customization kit produces high surgical accuracy in medial opening wedge high tibial osteotomy: a pilot study
Abstract
Purpose: Contemporary medial opening wedge high tibial osteotomy (MOWHTO) still seems to struggle with inconsistent accuracy outcomes. Our objective was to assess surgical accuracy and short-term clinical outcomes when using 3D planning and a patient-specific instrumentation (PSI) kit to prepare customized bone allografts.
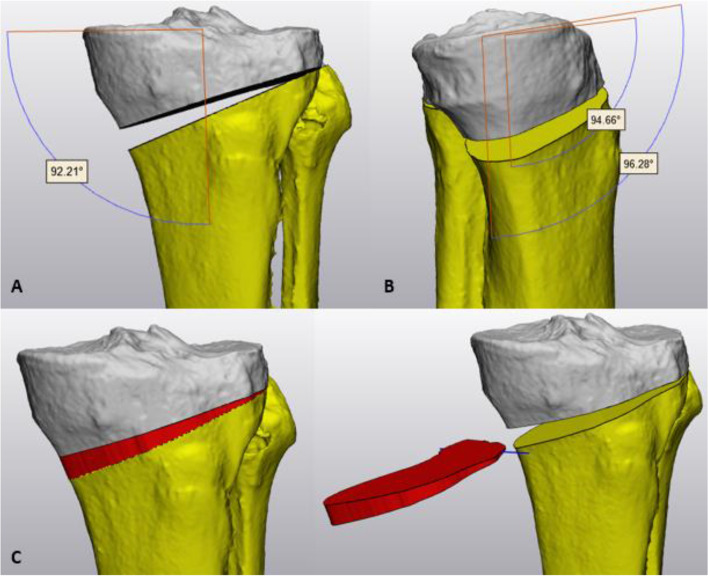
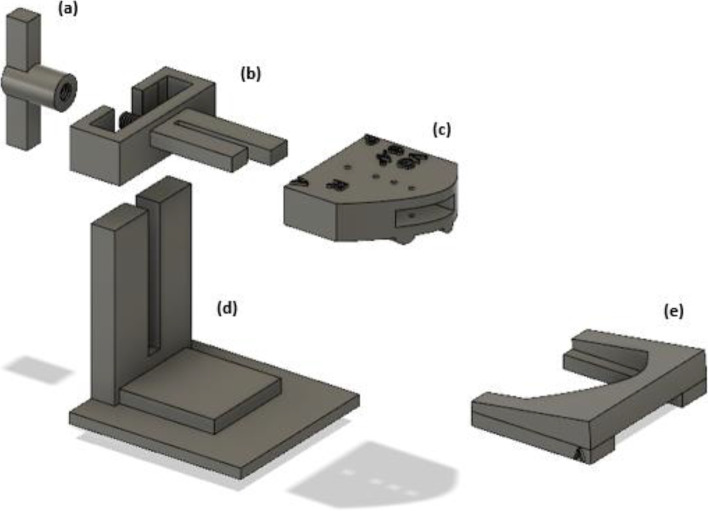
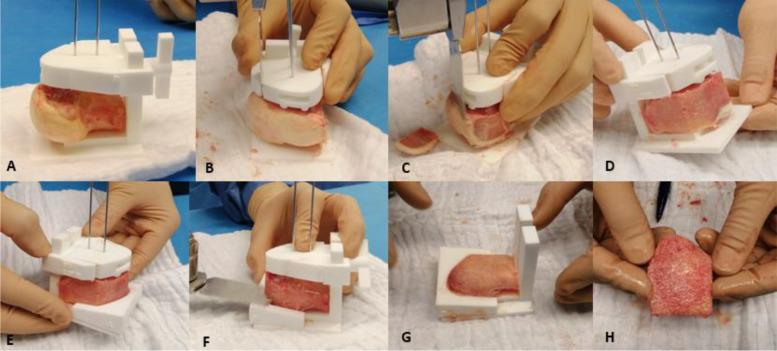
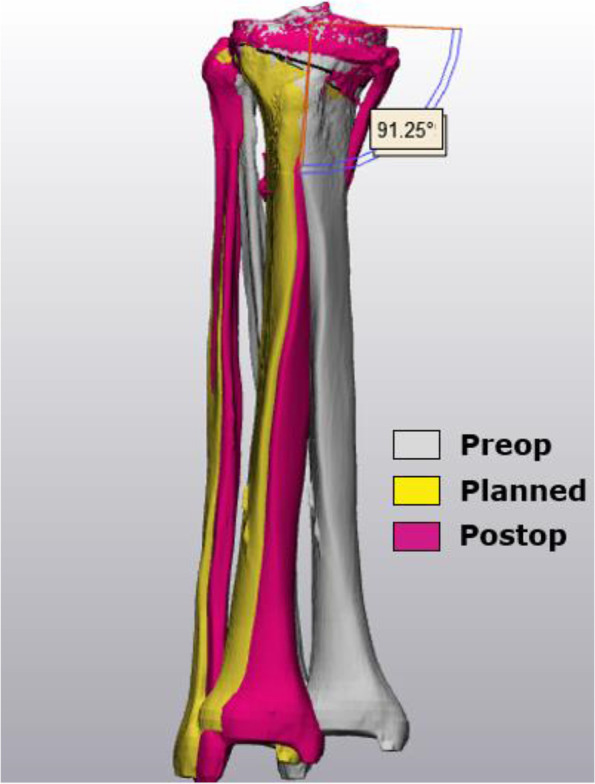
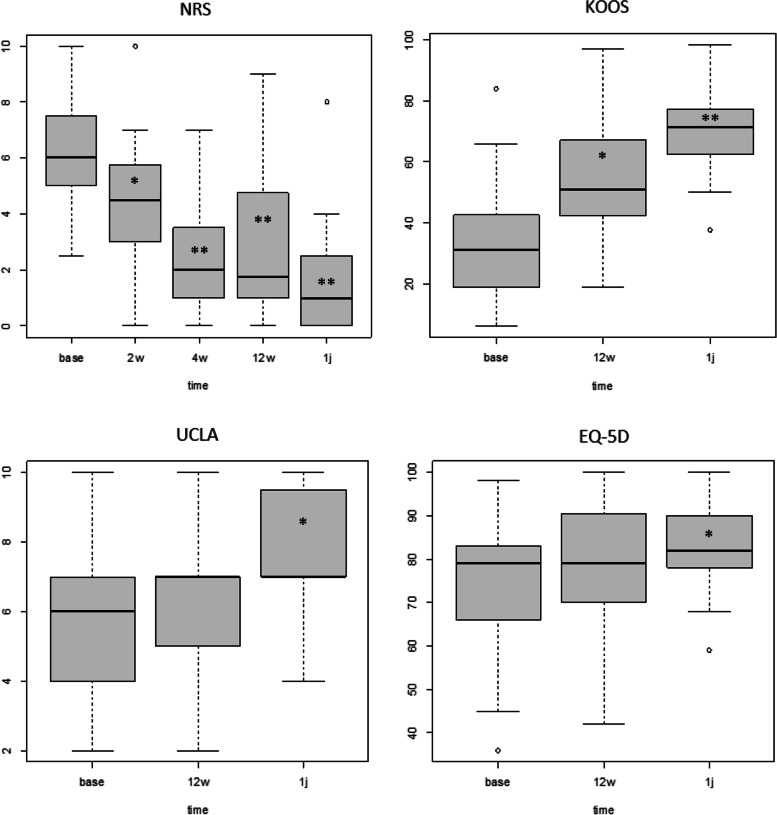
Methods: Thirty subjects (age 48y ± 13) were included in a double-center prospective case series. A low-dose CT-scan was performed to generate 3D bone models, a MOWHTO was simulated, and PSI was designed and 3D printed based on the complementary negative of the planned osteotomy gap. Clinical outcome was assessed at two, four, 12 weeks and one year using NRS, KOOS, UCLA activity score, EQ-5D and anchor questions. A linear-mixed model approach was implemented for data analysis.
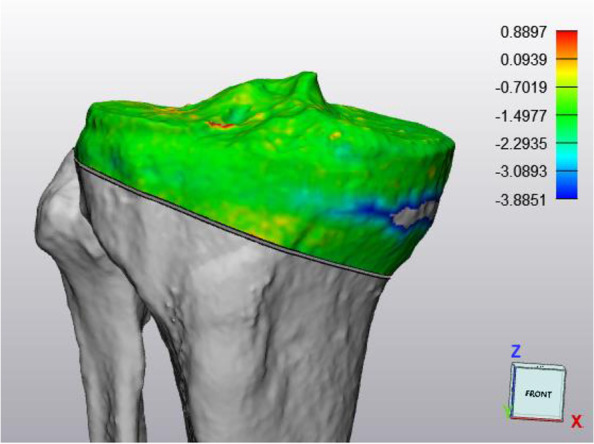
Results: Preoperative 3D values were 175.0° ± 2.2 mechanical tibiofemoral angle (mTFA), 85.0° ± 3.0 medial proximal tibial angle (MPTA), and 94.1° ± 3.4 medial posterior tibial slope (MPTS). Target planning ranged from slight varus to the lateral tibial spine (slight valgus). Postoperative 3D analysis showed an accuracy of 1.1° ± 0.7 ΔMPTA (p = 0.04) and 1.2° ± 1.2 ΔMPTS (p = 0.11). NRS decreased from baseline 6.1 ± 1.9 to 2.7 ± 1.9 at four weeks (p < 0.001) and 1.7 ± 1.9 at one year (p < 0.001). KOOS increased from 31.4 ± 17.6 to 50.6 ± 20.6 at 12 weeks (p < 0.001) and to 71.8 ± 15.6 at one year (p < 0.001).
Conclusion: The study suggests that 3D printed instrumentation to personalize structural bone allograft is a viable alternative method in MOWHTO that has the benefit of optimizing surgical accuracy while providing early and consistent pain relief after surgery.
Keywords: 3D planning; Accuracy; High tibial osteotomy; Joint preservation; Patient-specific instrumentation.
© 2023. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Van den Bempt M, Van Genechten W, Claes T, Claes S. How accurately does high tibial osteotomy correct the mechanical axis of an arthritic varus knee? A systematic review Knee. 2016;23(6):925–935. - PubMed
-
- Takagawa S, Kobayashi N, Yukizawa Y, Oishi T, Tsuji M, Inaba Y. Preoperative soft tissue laxity around knee was associated with less accurate alignment correction after hybrid closed-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(9):3022–3030. doi: 10.1007/s00167-019-05762-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
