

Association of Four Types of Vascular Access Including Arterial Superficialization with Mortality in Maintenance Hemodialysis Patients: A Nationwide Cohort Study in Japan
- PMID: 36917960
- PMCID: PMC11232950
- DOI: 10.1159/000529991
Association of Four Types of Vascular Access Including Arterial Superficialization with Mortality in Maintenance Hemodialysis Patients: A Nationwide Cohort Study in Japan
Abstract
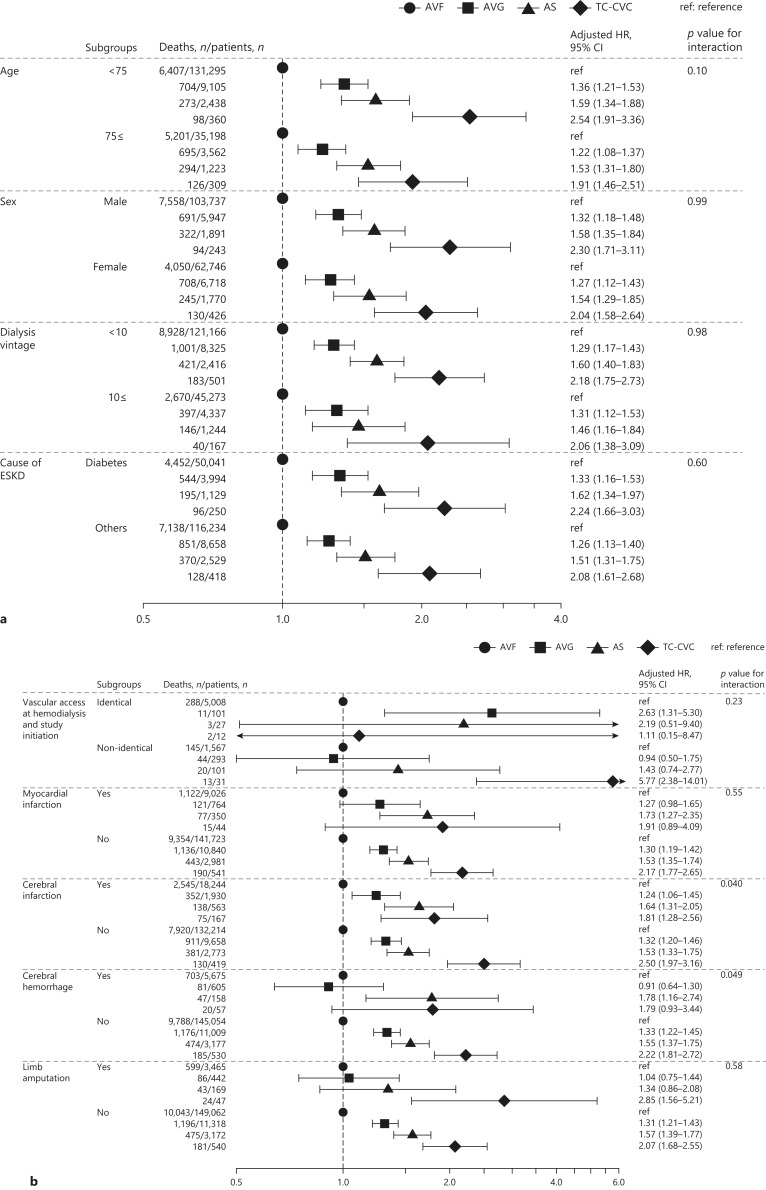
Introduction: Vascular access usage varies widely across countries. Previous studies have evaluated the association of clinical outcomes with the three types of vascular access, namely, arteriovenous fistula (AVF), arteriovenous graft (AVG), and tunneled and cuffed central venous catheter (TC-CVC). However, little is known regarding the association between arterial superficialization (AS) and the mortality of patients.
Methods: A nationwide cohort study was conducted using data from the Japanese Society for Dialysis Therapy Renal Data Registry (2006-2007). We included patients aged ≥20 years undergoing hemodialysis with a dialysis vintage ≥6 months. The exposures of interest were the four types of vascular access: AVF, AVG, AS, and TC-CVC. Cox proportional hazard models were used to evaluate the associations of vascular access types with 1-year all-cause and cause-specific mortality.
Results: A total of 183,490 maintenance hemodialysis patients were included: 90.7% with AVF, 6.9% with AVG, 2.0% with AS, and 0.4% with TC-CVC. During the 1-year follow-up period, 13,798 patients died. Compared to patients with AVF, those with AVG, AS, and TC-CVC had a significantly higher risk of all-cause mortality after adjustment for confounding factors: adjusted hazard ratios (95% confidence intervals) - 1.30 (1.20-1.41), 1.56 (1.39-1.76), and 2.15 (1.77-2.61), respectively. Similar results were obtained for infection-related and cardiovascular mortality.
Conclusion: This nationwide cohort study conducted in Japan suggested that AVF usage may have the lowest risk of all-cause mortality. The study also suggested that the usage of AS may be associated with better survival rates compared to those of TC-CVC in patients who are not suitable for AVF or AVG.
Keywords: Arterial superficialization; Arteriovenous fistula; Arteriovenous graft; Central venous catheter; Vascular access.
© 2023 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
N.F. has received personal fees from Chugai Pharmaceutical, Kissei Pharmaceutical, Kyowa Kirin, Ono Pharmaceutical, and Sanwa Kagaku Kenkyusho. T.H. has received personal fees from Chugai Pharmaceutical, Kissei Pharmaceutical, Kyowa Kirin, Ono Pharmaceutical, and Sanwa Kagaku Kenkyusho; and grants from Chugai Pharmaceutical, Kissei Pharmaceutical, Kyowa Kirin, and Ono Pharmaceutical. I.M. has received personal fees from Chugai Pharmaceutical, Kyowa Kirin, and Ono Pharmaceutical. No other authors have no conflicts of interest to declare.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
