

The clinical-radiological paradox in multiple sclerosis: myth or truth?
- PMID: 36918008
- PMCID: PMC10014204
- DOI: 10.1055/s-0042-1758457
The clinical-radiological paradox in multiple sclerosis: myth or truth?
Abstract
Background: Multiple sclerosis (MS) is an inflammatory, degenerative, demyelinating disease that ranges from benign to rapidly progressive forms. A striking characteristic of the disease is the clinical-radiological paradox.
Objectives: The present study was conducted to determine whether, in our cohort, the clinical-radiological paradox exists and whether lesion location is related to clinical disability in patients with MS.
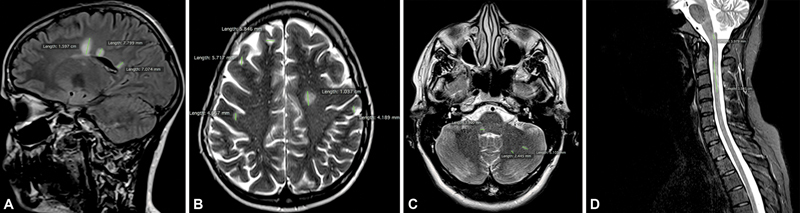
Methods: Retrospective data from 95 patients with MS (60 women and 35 men) treated at a single center were examined. One head-and-spine magnetic resonance imaging (MRI) examination from each patient was selected randomly, and two independent observers calculated lesion loads (LLs) on T2/fluid attenuation inversion recovery sequences manually, considering the whole brain and four separate regions (periventricular, juxtacortical, posterior fossa, and spinal cord). The LLs were compared with the degree of disability, measured by the Kurtzke Expanded Disability Status Scale (EDSS), at the time of MRI examination in the whole cohort and in patients with relapsing-remitting (RR), primarily progressive, and secondarily progressive MS.
Results: High LLs correlated with high EDSS scores in the whole cohort (r = 0.34; p < 0.01) and in the RRMS group (r = 0.27; p = 0.02). The EDSS score correlated with high regional LLs in the posterior fossa (r = 0.31; p = 0.002) and spinal cord (r = 0.35; p = 0.001).
Conclusions: Our results indicate that the clinical-radiological paradox is a myth and support the logical connection between lesion location and neurological repercussion.
Antecedentes: A esclerose múltipla (EM) é uma doença inflamatória, degenerativa e desmielinizante que varia de formas benignas a rapidamente progressivas. Uma característica marcante da doença é o paradoxo clínico-radiológico.
Objetivos: O presente estudo foi realizado para determinar, se na nossa amostragem, o paradoxo clínico-radiológico existe e se a localização das lesões está relacionada à incapacidade clínica em pacientes com EM. MéTODOS: Foram examinados retrospectivamente dados de 95 pacientes com EM (60 mulheres e 35 homens) atendidos em um único centro. Um exame de ressonância magnética de cada paciente foi selecionado aleatoriamente, e dois observadores independentes calcularam as cargas lesionais (CLs) em sequências T2 e FLAIR manualmente, considerando todo o cérebro e quatro regiões separadamente (periventricular, justacortical, fossa posterior e medula espinhal). As CLs foram comparadas com o grau de incapacidade, medido pela Escala de Status expandido de incapacidade (EDSS, na sigla em inglês) de Kurtzke, no momento do exame de ressonância magnética (RM) em toda a coorte e em pacientes com as formas surto remissão (SR), primariamente progressiva (PP), e secundariamente progressiva (SP) da EM.
Resultados: Cargas lesionais elevadas foram correlacionadas com altos índices de EDSS considerando toda a coorte (r = 0.34; p < 0.01) e no grupo SR (r = 0.27; p = 0.02). O EDSS foi correlacionado com CLs altas na fossa posterior (r = 0.31; p = 0.002) e na medula (r = 0.35; p = 0.001). CONCLUSõES: Nossos resultados indicam que o paradoxo clínico-radiológico é um mito e apoiam a conexão lógica entre a localização da lesão e a repercussão neurológica.
Academia Brasileira de Neurologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
The authors have no conflict of interests to declare.
Figures
References
-
- Lumsden C E.The neuropathology of multiple sclerosis Amsterdam: North-Holland Publishing Company, pp 217 ± 309.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical