

Society for Immunotherapy of Cancer (SITC) consensus definitions for resistance to combinations of immune checkpoint inhibitors with targeted therapies
- PMID: 36918225
- PMCID: PMC10016252
- DOI: 10.1136/jitc-2022-005923
Society for Immunotherapy of Cancer (SITC) consensus definitions for resistance to combinations of immune checkpoint inhibitors with targeted therapies
Abstract
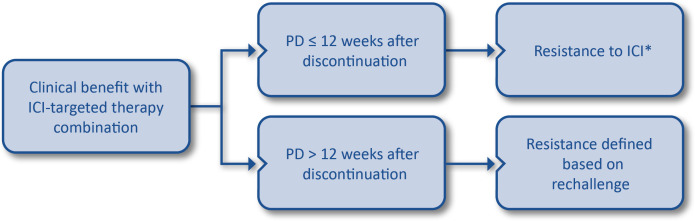
Immunotherapy offers deep and durable disease control to some patients, but many tumors do not respond to treatment with single-agent immune checkpoint inhibitors (ICIs). One strategy to enhance responses to immunotherapy is via combinations with signal transduction inhibitors, such as antiangiogenic therapies, which not only directly target cancer cells but also could potentially favorably modulate the tumor immune microenvironment. Combination strategies with ICIs have demonstrated enhanced antitumor activity compared with tumor-targeted or antiangiogenic therapy alone in randomized trials in a variety of solid tumor settings, leading to regulatory approval from the US Food and Drug Administration and agencies in other countries for the treatment of endometrial cancer, kidney cancer, melanoma, and hepatocellular carcinoma. Despite improved survival and response rates for some patients when antiangiogenic or targeted therapies are administered with ICIs, many patients continue to progress after combination treatment and urgently need new strategies to address this manifestation of resistance to immunotherapy. Previously, the Society for Immunotherapy of Cancer (SITC) published consensus definitions for resistance to single-agent anti-PD-(L)1. To provide guidance for clinical trial design and to support analyses of emerging molecular and immune profiling data surrounding mechanisms of resistance to ICI-based combinations, SITC convened a follow-up workshop in 2021 to develop consensus definitions for resistance to multiagent ICI combinations. This manuscript reports the consensus clinical definitions for combinations of anti-PD-(L)1 ICIs and targeted therapies. Definitions for resistance to ICIs in combination with chemotherapy and with other ICIs will be published in companion volumes to this paper.
Keywords: Clinical Trials as Topic; Drug Therapy, Combination; Guidelines as Topic; Immunotherapy; Tumor Escape.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MBA—Consulting fees: Aveo, Bristol Myers Squibb, Eisai, Exelixis, Genentech, Iovance, Merck, Novartis, Pfizer, Roche, Pyxis, Werewolf, Asher Bio, Calithera, Idera, Agenus, Apexigen, Neoleukin, Adagene, AstraZeneca, Elpis, ScholarRock, Surface, ValoHealth, Sanofi, Fathom; Ownership interest less than 5%: Werewolf, Pyxis, Elpis. DF—Salary and employment: Palleon Pharmaceuticals; Ownership interest less than 5%: Palleon Pharmaceuticals. DBJ—IP rights: MHC-II for use as immunotherapy biomarker, Abatacept as treatment for irAEs; Consulting fees: Bristol Myers Squibb, Catalyst, Iovance, Jansen, Mallinckrodt, Merck, Mosaic ImmunoIngineering, Novartis, Oncosec, Pfizer, Targovax; Contracted research: Bristol Myers Squibb, Incyte. JS—Consulting fees: Array, Nektar, Jazz, Iovance, Apexigen, Eisai; Contracted research: Bristol Myers Squibb, Amphivena, PACT. NIK—Consulting fees: Bristol Myers Squibb, Merck, Jounce, Iovance, Regeneron, Genzyme, NCCN (via Pfizer), Novartis, Nektar, Castle Biosciences, Instil Bio, Immunocore; Contracted research: Bristol Myers Squibb, Merck, Celgene, GSK, HUYA, Replimune, Novartis, Regeneron, Amgen; Data safety Montioring board: AstraZeneca, Incyte; Study steering committee: Nektar, Bristol Myers Squibb, Regeneron, Replimune; Ownership interest less than 5%: Bellicum Pharaceuticals, Asensus Surgical (formerly TransEnterix), Amarin. PAA—Consulting fees: Bristol Myers Squibb, Roche, Array, Novartis, Merck Serono, Pierre Fabre, Incyte, Medimmune, AstraZeneca, Sun Pharma, Sanofi, Idera, Sandox, Immunocore, 4SC, Italfarmaco, Mektar, Boehringer Ingelheim, Eisai, Renegeron, Daiichi Sankyo, Pfizer, Oncosec, Nouscom, Lunaphore, SeaGen, iTEOS, Medicenna; Contracted research: Bristol Myers Squibb, Genentech/Roche, Array, Sanofi. TAY—Consulting fees: AstraZeneca, Almac, Aduro, Artios, Athena, Atrin, Axiom, Bayer, Bristol Myers Squibb, Calithera, Clovis, Cybrexa, EMD Serono, F-Star, GLG, Guidepoint, Ignyta, I-Mab, ImmuneSensor, Jansen, Merck, Pfizer, Repare, Roche, Schrodinger, Seattle Genetics, Varian, Zai Labs, ZielBio; Contracted research: AstraZeneca, Artios, Bayer, Beigene, BioNTech, Bristol Myers Squibb, Clovis, Constellation, Cyteir, Eli Lilly, EMD Serono, Forbius, F-Star, GlaxoSmithKline, Genentech/Roche, Haihe, ImmuneSensor, Ionis, Ipsen, Jounce, Karyopharm, KSQ, Kyowa, Merck, Novartis, Pfizer, Repare, Ribon Therapeutics, Regeneron, Rubius, Sanofi, Scholar Rock, Seattle Genetics, Tesaro, Vivace. HK—Consulting fees: Iovance, Immunocore, Celldex, Array Biopharma, Merck, Elevate Bio, Instil Bio, Bristol Myers Squibb, Clinigen, Shionogi, Chemocentryx, Calithera, Signatero. RJS—Consulting fees: Asana Biosciences, AstraZeneca, Bristol Myers Squibb, Eisai, Iovance, Merck, Novartis, OncoSec, Pfizer, Replimune; Contracted research: Merck, Amgen. HT—Consulting fees: Genentech/Roche, Bristol Myers Squibb, Novartis, Merck, Pfizer, Eisai, Karyopharm, Boxer Capital; Contracted research: Genentech/Roche, Bristol Myers Squibb, Novartis, Merck, GSK. JLG—Nothing to disclose. SITC Staff: SMW, PI—Nothing to disclose.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical