

Sequential Organ Failure Assessment (SOFA) Score for predicting mortality in patients with sepsis in Vietnamese intensive care units: a multicentre, cross-sectional study
- PMID: 36918251
- PMCID: PMC10016261
- DOI: 10.1136/bmjopen-2022-064870
Sequential Organ Failure Assessment (SOFA) Score for predicting mortality in patients with sepsis in Vietnamese intensive care units: a multicentre, cross-sectional study
Abstract
Objectives: To compare the accuracy of the Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II (APACHE II) Scores in predicting mortality among intensive care unit (ICU) patients with sepsis in a low-income and middle-income country.
Design: A multicentre, cross-sectional study.
Setting: A total of 15 adult ICUs throughout Vietnam.
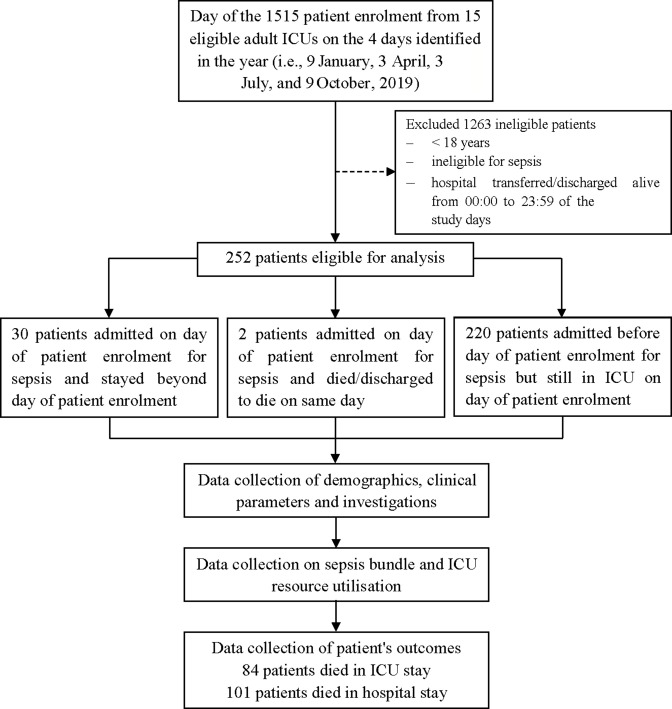
Participants: We included all patients aged ≥18 years who were admitted to ICUs for sepsis and who were still in ICUs from 00:00 to 23:59 of the specified study days (ie, 9 January, 3 April, 3 July and 9 October of the year 2019).
Primary and secondary outcome measures: The primary outcome was hospital all-cause mortality (hospital mortality). We also defined the secondary outcome as all-cause deaths in the ICU (ICU mortality).
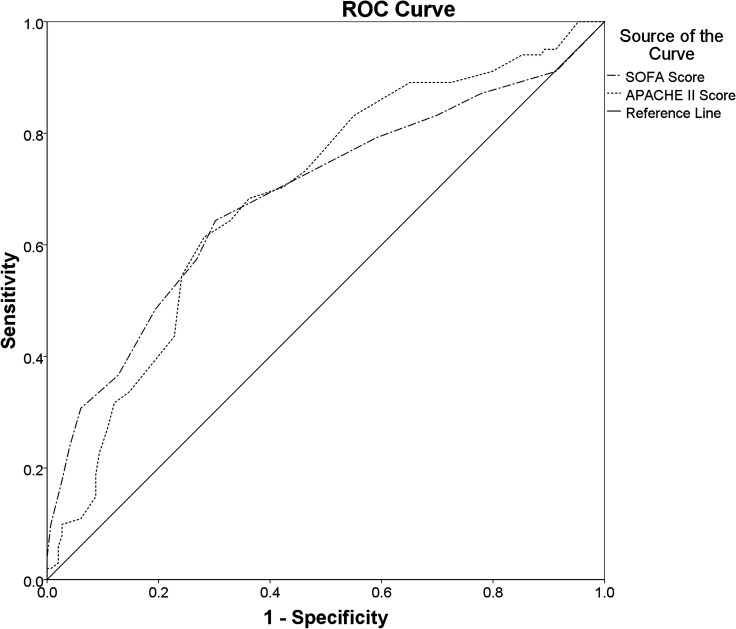
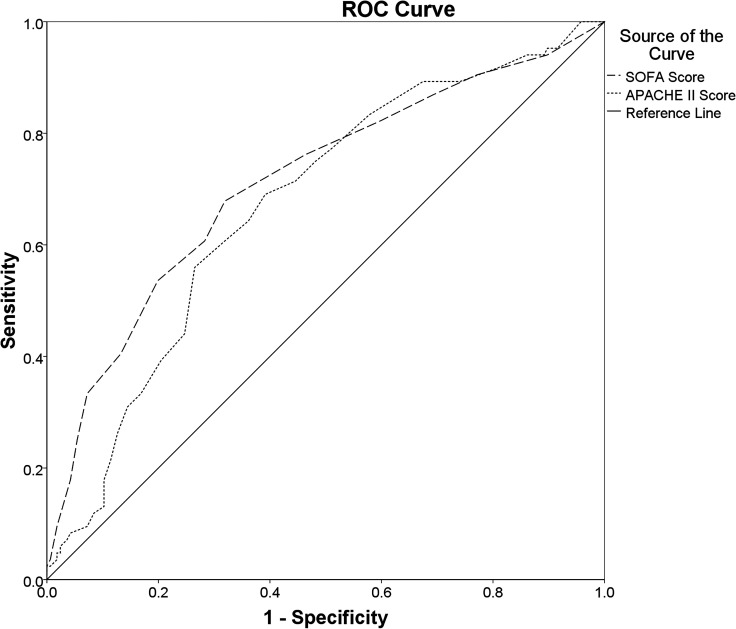
Results: Of 252 patients, 40.1% died in hospitals, and 33.3% died in ICUs. SOFA Score (areas under the receiver operating characteristic curve (AUROC): 0.688 (95% CI 0.618 to 0.758); cut-off value≥7.5; PAUROC<0.001) and APACHE II Score (AUROC: 0.689 (95% CI 0.622 to 0.756); cut-off value ≥20.5; PAUROC<0.001) both had a poor discriminatory ability for predicting hospital mortality. However, the discriminatory ability for predicting ICU mortality of SOFA (AUROC: 0.713 (95% CI 0.643 to 0.783); cut-off value≥9.5; PAUROC<0.001) was fair and was better than that of APACHE II Score (AUROC: 0.672 (95% CI 0.603 to 0.742); cut-off value≥18.5; PAUROC<0.001). A SOFA Score≥8 (adjusted OR (AOR): 2.717; 95% CI 1.371 to 5.382) and an APACHE II Score≥21 (AOR: 2.668; 95% CI 1.338 to 5.321) were independently associated with an increased risk of hospital mortality. Additionally, a SOFA Score≥10 (AOR: 2.194; 95% CI 1.017 to 4.735) was an independent predictor of ICU mortality, in contrast to an APACHE II Score≥19, for which this role did not.
Conclusions: In this study, SOFA and APACHE II Scores were worthwhile in predicting mortality among ICU patients with sepsis. However, due to better discrimination for predicting ICU mortality, the SOFA Score was preferable to the APACHE II Score in predicting mortality.Clinical trials registry - India: CTRI/2019/01/016898.
Keywords: ACCIDENT & EMERGENCY MEDICINE; Adult intensive & critical care; BACTERIOLOGY; INTENSIVE & CRITICAL CARE.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2013: statistical brief #204. In: Knutson D, ed. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US), 2006. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous