

Crimean-Congo haemorrhagic fever virus
- PMID: 36918725
- PMCID: PMC10013989
- DOI: 10.1038/s41579-023-00871-9
Crimean-Congo haemorrhagic fever virus
Abstract
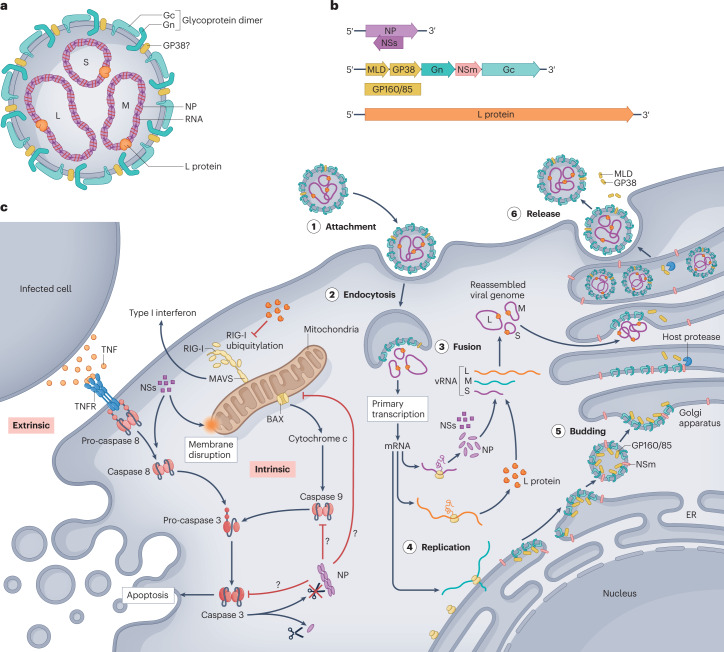
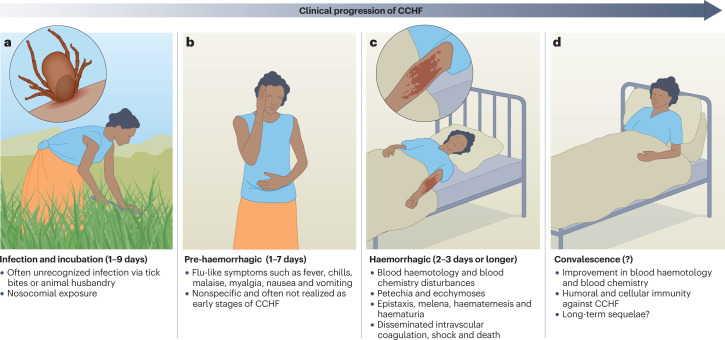
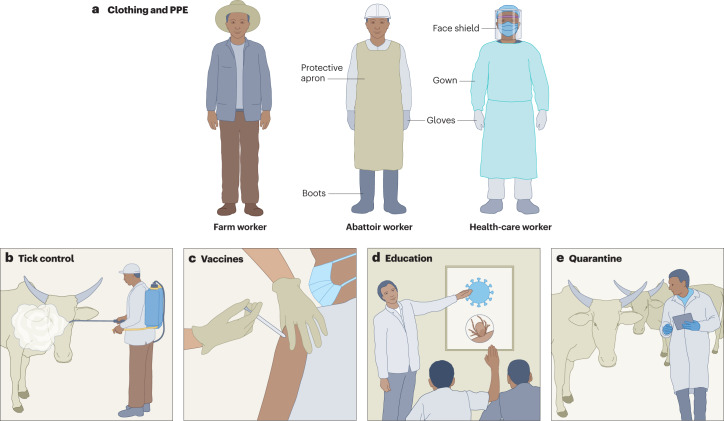
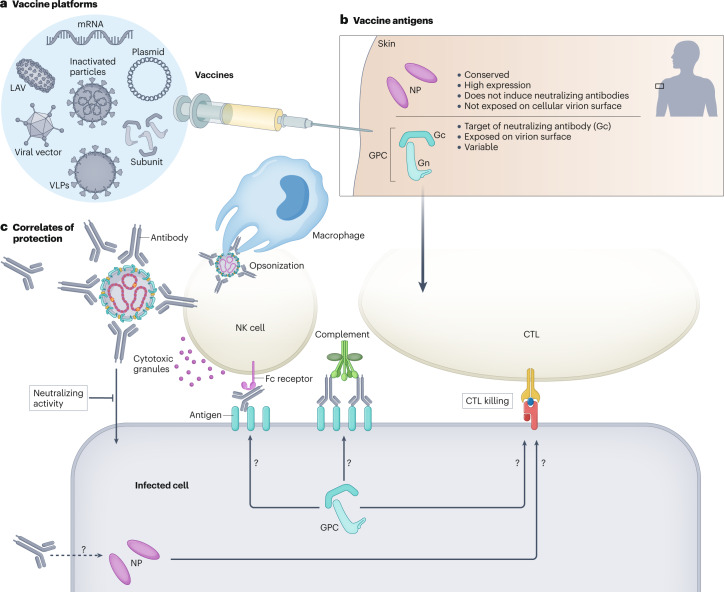
Crimean-Congo haemorrhagic fever (CCHF) is a severe tick-borne illness with a wide geographical distribution and case fatality rates of 30% or higher. Caused by infection with the CCHF virus (CCHFV), cases are reported throughout Africa, the Middle East, Asia and southern and eastern Europe. The expanding range of the Hyalomma tick vector is placing new populations at risk for CCHF, and no licensed vaccines or specific antivirals exist to treat CCHF. Furthermore, despite cases of CCHF being reported annually, the host and viral determinants of CCHFV pathogenesis are poorly understood. CCHFV can productively infect a multitude of animal species, yet only humans develop a severe illness. Within human populations, subclinical infections are underappreciated and may represent a substantial proportion of clinical outcomes. Compared with other members of the Bunyavirales order, CCHFV has a more complex genomic organization, with many viral proteins having unclear functions in viral pathogenesis. In recent years, improved animal models have led to increased insights into CCHFV pathogenesis, and several antivirals and vaccines for CCHFV have shown robust efficacy in preclinical models. Translation of these insights and candidate therapeutics to the clinic will hopefully reduce the morbidity and mortality caused by CCHFV.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
D.W.H. and H.F. are listed as inventors on US patent application number 63/365,015 ‘Replicating RNA vaccine for Crimean–Congo hemorrhagic fever virus’.
Figures
References
-
- Simpson DI, et al. Congo virus: a hitherto undescribed virus occurring in Africa. I. Human isolations–clinical notes. East Afr. Med. J. 1967;44:86–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
