

Modified Dynamic Conformal Arcs With Forward Planning for Radiosurgery of Small Brain Metastasis: Each Double Arc and Different To-and-Fro Leaf Margins to Optimize Dose Gradient Inside and Outside the Gross Tumor Boundary
- PMID: 36919061
- PMCID: PMC10008411
- DOI: 10.7759/cureus.34831
Modified Dynamic Conformal Arcs With Forward Planning for Radiosurgery of Small Brain Metastasis: Each Double Arc and Different To-and-Fro Leaf Margins to Optimize Dose Gradient Inside and Outside the Gross Tumor Boundary
Abstract
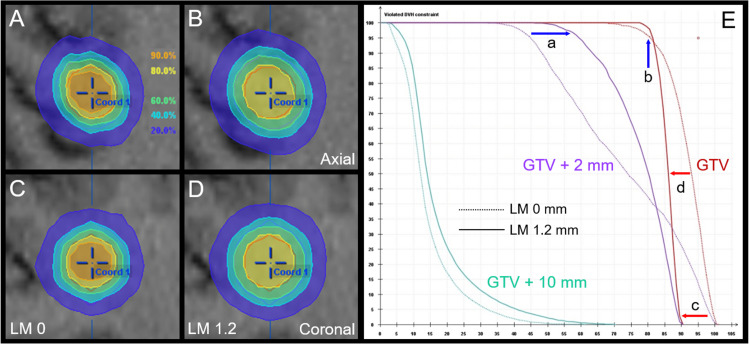
Dynamic conformal arcs (DCA) are a widely used technique for stereotactic radiosurgery (SRS) of brain metastases (BM) using a micro-multileaf collimator (mMLC), while the planning design and method considerably vary among institutions. In the usual forward planning of DCA, the steepness of the dose gradient outside and inside the gross tumor volume (GTV) boundary is simply defined by the leaf margin (LM) setting to the target volume edge. The dose fall-off outside the small GTV tends to be excessively precipitous, especially with an MLC of 2.5-mm leaf width, which is predisposed to the insufficient coverage of microscopic brain invasion and other inherent inaccuracies. Meanwhile, insufficient dose increase inside the GTV boundary, i.e., less inhomogeneous GTV dose, likely leads to inferior and less sustainable tumor response. The more inhomogeneous GTV dose is prone to the steeper dose gradient outside the GTV and vice versa. Herein, we describe an alternative simply modified DCA (mDCA) planning that was uniquely devised to optimize the dose gradient outside and inside the GTV boundary for further enhancing and consolidating local control of small BM. For a succinct exemplification, a 10-mm spherical target was assumed as a GTV for DCA planning using a 2.5-mm mMLC. The benchmark plan was generated by adding a 0-mm LM to the GTV edge by assigning a single fraction of 30 Gy to the isocenter, in which the GTV coverage by 24 Gy with 80% isodose surface (IDS) was 96%, i.e., D96%, while the coverage of GTV + isotropic 2 mm volume by 18 Gy with 60% IDS was 70%, with the D98% being 12 Gy with 40% IDS, viz., too steep dose fall-off outside the GTV boundary. Alternatively, the increase of LM with or without decreasing the isocenter dose enables the increase of the GTV + 2 mm coverage by 18 Gy while resulting in an inadequate GTV dose with either a less inhomogeneous dose or an excessive marginal dose. Meanwhile, in the newly devised mDCA planning, every single arc was converted to a double to-and-fro arc with different LM settings under the same spatial arrangement, which enabled GTV + 2 mm volume coverage with 18 Gy while preserving the GTV marginal dose and inhomogeneity similar to those for the benchmark plan. Additionally, the different collimator angle (CA) setting for the to-and-fro arcs led to further trimming of the dose conformity. The limitations of general forward planning with only adjusting the LM for every single arc were demonstrated, which can be a contributing factor for local tumor progression of small BM. Alternatively, the mDCA with each double to-and-fro arc and different LM and CA settings enables optimization of the dose gradient both outside and inside the GTV boundary according to the planners' intent, e.g., moderate dose spillage margin outside the GTV and steep dose increase inside the GTV boundary.
Keywords: brain invasion; brain metastasis; dose distribution; dose gradient; dose inhomogeneity; dynamic conformal arcs; forward planning; micro-multileaf collimator; small tumor; stereotactic radiosurgery.
Copyright © 2023, Ohtakara et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- ISRS technical guidelines for stereotactic radiosurgery: Treatment of small brain metastases (≤1 cm in diameter) Grishchuk D, Dimitriadis A, Sahgal A, et al. Pract Radiat Oncol. 2022 - PubMed
-
- Significance of target location relative to the depth from the brain surface and high-dose irradiated volume in the development of brain radionecrosis after micromultileaf collimator-based stereotactic radiosurgery for brain metastases. Ohtakara K, Hayashi S, Nakayama N, Ohe N, Yano H, Iwama T, Hoshi H. J Neurooncol. 2012;108:201–209. - PubMed
-
- The incidence and its associated factors relevant to brain radionecrosis that requires intervention following single or fractionated stereotactic radiosurgery using vero4DRT for brain metastases. Yamada T, Ohtakara K, Kamomae T, Itoh J, Shimada H, Ishihara S, Naganawa S. Cureus. 2022;14:0. - PMC - PubMed
LinkOut - more resources
Full Text Sources